

A multi-disciplinary, transtheoretical guide to developing and leading psychotherapy groups, addressing areas considered essential to the successful practice of group psychotherapy. Supported by clinical research, and developed through an expert consensus process, they are a practical resource for mental health professionals, and also serve the public-at-large by providing consumers with valuable information on the practice of group psychotherapy. They are a concise guide to the basic tenets of practice, with a client-centered approach that maintains clinical integrity and creativity.”
Overview and Use of Practice Guidelines for Group Psychotherapy
Molyn Leszcz, MD, CGP, AGPA-DF discusses the content of the Practice Guidelines for Group Psychotherapy developed by AGPA and how to use them in clinical practice and training settings.
Preface
It is a pleasure both personally and on behalf of the American Group Psychotherapy Association (AGPA) to provide a preface for this important document.
This thoughtful, scholarly document has been developed by a blue ribbon Science to Service Task Force under the talented leadership of Molyn Leszcz, M.D. FRCPC, CGP, and Joseph C. Kobos, Ph.D, ABPP, CGP, FAGPA. The Task Force was assembled in an effort to bridge the gap in the group psychotherapy field between research and clinical practice. The guiding thought was that developing a heightened awareness and capacity for integrating science with ongoing clinical practice is not only consistent with national trends in health services, but also a useful means for persuasively demonstrating the effectiveness of group psychotherapy and for improving the quality of care that is being delivered.
The Task Force was given the following broad charge: (1) formulating a relevant and useful set of practice guidelines for group psychotherapy; (2); building atop the seminal work of the CORE – R Battery Task Force by field testing the CORE-R Battery (Burlingame et al., 2006) and then supporting its wider implementation (3) developing a practice-research network; and (4) supporting AGPA’s commitment to its membership and to the field to accrue and demonstrate evidence for the effectiveness of group psychotherapy.
This compilation of practice guidelines that follows constitutes our first integrated organizational response to address the challenge and growing demand for accountability. By incorporating research findings as the bedrock for developing these guidelines, AGPA is seizing the initiative on behalf of both providers and consumers to establish more firmly evidence-based practices for conducting effective group psychotherapy.
All of AGPA can take pride in this important contribution. Assembling this comprehensive set of practice guidelines, coupled with a set of assessment tools to permit careful, standardized evaluations and feedback for ongoing clinical intervention, constitutes a giant leap forward for us and for the field of group psychotherapy.
Robert H. Klein, Ph.D., ABPP, CGP, LFAGPA
Introduction
In 2008, the American Group Psychotherapy Association (AGPA) published a seminal document that was described as a “giant leap forward for us and for the field of group psychotherapy” (Klein, 2008): The Clinical Practice Guidelines for Group Psychotherapy (Bernard et al., 2008). The guidelines were the product of years of work by the AGPA Science to Service Task Force, under the leadership of Molyn Leszcz, M.D., FRCPC, CGP, and Joseph Kobos, Ph.D., ABPP, CGP, AGPA-F. The Task Force was created with the goal of bridging the gap between group psychotherapy research and clinical practice. Its primary objective was to create a set of evidence-based practice guidelines based on the group psychotherapy literature that would support clinicians in their implementation of group interventions (Klein, 2008). That goal was met successfully.
The 2008 Clinical Practice Guidelines were the first resource of this kind produced by the AGPA and their purpose was clearly outlined. In their introduction, the authors differentiated them from practice standards by noting their flexibility and aspirational nature. They stated that the guidelines were meant to be “broader and aspirational rather than narrow, prescriptive, and mandatory” (p. 457). This distinction underscored their main purpose: creating a supportive resource for clinicians and not a set of required standards to implement rigidly. Adopting a client-based approach to evidence-based practice, this goal was met by integrating available “empirical and clinical-theoretical literatures” (p. 457) and clinical practice (Bernard et al., 2008). By doing so, the Task Force assembled a foundational guide to support therapists’ group practice.
The Practice Guidelines were initially introduced on the AGPA website in 2007 and then published in 2008 as a special issue of the International Journal of Group Psychotherapy. Given the impressive number of downloads and citations, there is no question of the significant impact the guidelines have made in the group psychotherapy field, as a resource for clinicians, a training tool, and information available to the general population.
Purpose of the Update
In its introduction to the guidelines, the Science to Service Task Force noted that such a document should be considered a work in progress and that revisions and updates would be needed as new conceptualizations are developed and empirical findings discovered. Burlingame and Jensen (2017) highlighted that not only has the amount of group psychotherapy research significantly increased, the research available has also become more rigorous, providing clearer answers about processes involved in conducting successful groups. In fact, they stated that “group treatment has more solid research support for its efficacy now than at any time in its history” (p. s209) and suggested that the future of group research is as promising as what unfolded in the past three decades. This shows that our understanding of what makes group psychotherapy effective has broadened since the publication of the original guidelines. Integrating these research advances in this revision was an essential step to continue adequately supporting clinicians in an era of evidence-based treatment.
In addition to growth in our knowledge and understanding of group psychotherapy, it is important to recognize that the context in which therapists conduct groups has also increased since 2007. Over the past few decades, the willingness to engage with questions of multicultural competence and social justice in the field has also grown significantly. Professional organizations have emphasized the need for clinicians to increase their multicultural competence lest their treatments harm those who have been oppressed or devalued through the larger sociocultural forces in which treatments are embedded (Owen, et al., 2019). This body of research emphasizes the need for clinicians to engage in their practice with cultural humility, and to strive to continue increasing their knowledge, awareness, and skills in working with diverse individuals (Sue & Sue, 2012). In sum, the mental health field recognizes that “good counseling is culturally responsive counseling” (Sue, et al., 2022, p. 28).
Historically, group psychotherapy research, like the field of psychotherapy research as a whole, has neglected studying issues related to diversity and social justice (Frey, 2000). This negligence becomes especially obvious when comparing group and individual psychotherapy research (Chen et al., 2008). Eason, for example, pointed out a lack of focus on marginalized populations in the group psychotherapy research, as well as “hesitancy” to acknowledge the Eurocentricity of the field (Eason, 2009). Chen and colleagues (2008) also emphasized the lack of group psychotherapy research on diversity. Specifically, they noted that the AGPA Practice Guidelines did not sufficiently address “ways in which racial and cultural minority group members’ characteristics, values, preferences, and sociocultural context should be considered in promoting effective practice” (p. 1265). Thus, they emphasized the need for more research regarding multicultural practice and group psychotherapy, as well as the need for modifications to the guidelines to optimize outcomes for all populations (Chen et al., 2008).
Acknowledging that more research is needed to better understand the experiences of marginalized individuals in group psychotherapy is an important step. However, providing mental health services that adequately meet the needs of populations that hold marginalized identities requires more from therapists than simply increasing their knowledge and awareness of diverse experiences. Cultural competence is also a call to create services that are more equitable and that advocate for the same equity outside of the therapy room. This is particularly important in the current global sociopolitical context, where we are witnessing increased systemic erasure of and violence against marginalized groups. In other words, therapists can engage in social justice work by not limiting their work to the individual client or the group, but by advocating for change at the systemic level (Chen et al., 2008). Cultural competence and social justice have often been approached as less important and only supplemental to clinical work. However, they are increasingly understood to be fundamental aspects of our overall competence as therapists (Sue et al., 2022). Therefore, they should be fully integrated in each step of the therapeutic process. As Michele Ribeiro (2020) stated:
As therapists, we have the ethical and moral responsibility to understand not just the theories that guide our work (e.g., CBT, ACT, psychodynamic, etc.) but also the nuances within our work that are the hallmarks of what makes us unique and fundamentally connected. (p. xxv)
In a field that has primarily been rooted in White Western and European perspectives (Eason, 2009; Ribeiro, 2020; Thalmayer et al., 2021; Sue et al., 2022), we must be willing to name that the lack of focus on marginalized populations has caused harm and reduced trust in the services we provide (Sue et al., 2022). To create change and increase safety for clients from various backgrounds, we must acknowledge power, privilege, and oppression, and how they influence every aspect of our individual and interpersonal functioning. To be truly culturally competent, therapists must be able to understand past and present oppression and its impact (e.g., racism, xenophobia, sexism, heterosexism, ableism, religious oppression, classism, etc.). This is perhaps particularly true for group therapists. In their expansion of the Multicultural Orientation (MCO) model to group psychotherapy, Kivlighan and Chapman (2018) posit that “therapy groups are inherently multicultural” (p. 39). In fact, the group therapy literature has consistently highlighted that therapy groups are social microcosms of the external world. Scholars have argued that the outcomes of groups can be impacted by diverse group compositions; in a multicultural context, this means that privilege and oppression will inevitably manifest in groups (Chen et al., 2008). For instance, Kivlighan and Chapman (2018) noted that, in some groups, Black, Indigenous, and People of Color (BIPOC) had worse outcomes than White group members. Similarly, groups can be spaces where ableism, heterosexism, sexism, or other forms of oppression harm members. Research has shown that microaggressions occur in therapy groups and impact members’ perception of group cohesion (Kivlighan et al., 2021).
While groups have the potential to be spaces where marginalized members can experience reparative and healing experiences, this cannot happen without therapists’ awareness of how oppression manifests and their willingness to act to prevent harm. Therapists must, therefore, be aware of their own participation in such power dynamics (Ribeiro, 2020). Therapists must also be willing to understand how integrating and welcoming cultural values and identity in treatment settings can enhance clients’ experiences in positive ways. Group psychotherapy research underscores the unique role of group therapists and the potential power of therapy groups in creating reparative emotional experiences for their members. Therapists must, therefore, be informed about diverse forms of oppression, understand dynamics of power and privilege to be able to identify them when they manifest in groups, and commit to act. This involves being open to continually engage in learning about the unique experiences, values and beliefs of the clients that enter the group. Being prepared to pay particular attention to the present experiences of marginalized group members, creating space for them in the group, and addressing harm when it occurs is, therefore, essential (Ribeiro, 2020).
As noted by Chen and colleagues (2008), the 2008 AGPA Practice Guidelines did not provide the needed depth to these issues. Since their publication, so much progress has been made including, as we have noted, the constructions of a Multicultural Orientation model specifically for the therapy group and the group therapist. The AGPA has provided resources for clinicians and created task forces and special interest groups to try to create a more equitable organization (cf. Abernethy, 2024). The AGPA Diversity, Equity and Inclusion Task Force created a groundbreaking resource to support clinicians by producing Guidelines for Creating Affirming and Restorative Group Experiences (AGPA Diversity, Equity and Inclusion Task Force, 2023). Integrating such important contributions into the practice guidelines was an essential step of this update.
The Process
Acknowledging the burgeoning growth of both outcome and process research noted above and the need to develop multicultural skills, the Science to Service Task Force leadership, Les R. Greene, Ph.D., CGP, AGPA-DLF, and Rebecca MacNair-Semands, Ph.D., CGP, AGPA-F, initiated this update in 2020. They assigned Louise F. Wheeler, Ph.D., as the project editor and, together, they invited scholars and expert clinicians to contribute. These invitations were extended based on expertise and with insight provided by other scholars, clinicians, and some of AGPA Special Interest Groups (SIGs) chairs. As with many projects that were initiated in the midst of the COVID-19 pandemic, the guidelines update encountered several setbacks and interruptions that slowed its process down. Nevertheless, the team of authors who contributed committed significant time, labor, and energy to producing a document that would meet the current demand. Authors were paired and assigned sections of the guidelines to revise and update based on their expertise. The literature was thoroughly reviewed to ensure that the guidelines be as up to date as possible. Each section underwent multiple reviews by a group of expert reviewers, many of whom contributed to the original guidelines. The final document was assembled by the project lead, edited to meet editorial standards, and reviewed by the Science to Service Task Force leadership before being submitted for publication.
About the Update
The Clinical Practice Guidelines for Group Psychotherapy update has similar goals as its predecessor. Specifically, it aims to support therapists and meet the needs of group therapy members by providing evidence-based practice guidelines that are accessible and in line with current trends in the field. To do so, the revised guidelines provide an up-to-date review of the literature. They also take into account the importance of understanding clinical practice through a multicultural and social justice lens. Each section of the guidelines aims at integrating research and practical innovations on diversity and social justice and evidence-based clinical practice recommendations. And, like the original guidelines, this revision is intended to be used by clinicians across diverse theoretical frameworks, clinical settings, and patient populations.
As the authors and reviewers discussed ways to create a document as representative of the current state of the field as possible, different topics emerged that were not included in the initial document. For instance, more in-depth attention was given to issues related to co-leadership and training and group therapist competence. Furthermore, a new chapter was added on the topic of therapy groups held online to meet the demand for specialized training in this area.
The principles presented in the guidelines are consistent with other resources produced by AGPA, such as the AGPA Group Therapy Training and Practice Series, beginning with Core Principles of Group Psychotherapy (Kaklauskas & Greene, 2020) and five additional volumes that can be found on the Routledge website (https://www.routledge.com/AGPA-Group-Therapy-Training-and-Practice-Series/book-series/AGPA). It is our fervent hope that these revised and updated guidelines provide a solid evidence-based grounding for the practice of group psychotherapy for the betterment of all of our clients.
Science to Service Task Force Members
Harold Bernard, Ph.D., ABPP, CGP, DFAGPA, Clinical Associate Professor, Department of Psychiatry, New York University School of Medicine
Gary Burlingame, Ph.D., CGP, FAGPA Professor of Psychology, Brigham Young University
Phillip Flores, Ph.D., CGP, FAGPA, Adjunct Faculty at the Georgia School of Professional Psychology at Argosy University and Supervisor of Group Psychotherapy, Emory University, Atlanta, Georgia
Les Greene, Ph.D., CGP, FAGPA, Department of Psychology, VA Medical Center, Editor, International Journal of Group Psychotherapy
Anthony Joyce, Ph.D., CGP, Professor and Coordinator, Psychotherapy Research and Evaluation Unit, Department of Psychiatry, University of Alberta
Joseph C. Kobos, Ph.D., ABPP, CGP, FAGPA, Director, Counseling Service, Professor, Psychiatry, University of Texas Health Science Center, San Antonio (Co-Chair of Task Force)
Molyn Leszcz, MD, FRCPC, CGP, Psychiatrist-in-Chief, Department of Psychiatry, Mount Sinai Hospital, Associate Professor and Head, Group Psychotherapy, Department of Psychiatry, University of Toronto (Co-Chair of Task Force)
Rebecca R. MacNair-Semands, Ph.D., CGP, Associate Director and Group Therapy Coordinator, Counseling Center, University of North Carolina at Charlotte
William E. Piper, Ph.D., CGP, FAGPA, Professor and Head, Division of Behavioral Science, Director, Psychotherapy Program, Department of Psychiatry, University of British Columbia
Anne M. Slocum McEneaney, Ph.D., CGP, Eating Disorders Specialist and Clinical Psychologist, New York University Counseling Service
Diane Feirman, CAE, Public Affairs Director, American Group Psychotherapy Association, Task Force Liaison
Creating Successful Therapy Groups
Overview
Experienced group therapists know that many factors involved in making a therapy group successful occur even before group members meet and the group begins. Regardless of the settings in which a group is held (e.g., university counseling centers, private practices, outpatient and inpatient settings, hospital-based settings, or community centers), group leaders are faced with many administrative and clinical decisions that will impact a group’s outcomes long before it actually begins (Rutan, et al., 2020a; Turner, 2017). This chapter provides guidelines to support group leaders in the process of creating successful therapy groups and can be applied across theoretical frameworks and group types.
Group Specialty Practice
In 2018, the American Psychological Association (APA) recognized group psychotherapy as a specialized form of psychotherapy, indicating that its practice requires specific and advanced training. While this recognition only applied to the field of psychology, the need for specialized training across disciplines practicing group therapy is the same. Unfortunately, many training and clinical sites continue to neglect training in this area, sending clinicians into the field with limited understanding of what is involved in group psychotherapy (Whittingham, et al., 2021). Acknowledging the need for specialized training is essential to equip clinicians with the knowledge and tools to create and run groups that will best serve their clients. As Barlow (2013) emphasizes:
Expected or unpredictable group events, group members’ worries about the possible disadvantages of groups, and advantages of groups can be dealt with by utilizing appropriate education and training of group leaders. Good leader training makes it possible for the disadvantages to be minimized and the advantages to be maximized. (p.6)
Training programs have a responsibility to provide adequate and specialized training to their students as learning to create and run effective therapy groups involves becoming familiar with new and unique skills, as well as “unlearning” other skills and frameworks (Barlow, 2013; Whittingham, et al., 2021). Such training should involve in-depth study of the group therapy literature and best practice guidelines, introduction to concepts and practice of skills unique to group psychotherapy and group case conceptualization, introduction to assessment measures specific to group, and awareness of professional organizations devoted to the study and practice of group psychotherapy. Clinicians should graduate from their training programs able to identify the different types of groups and the theoretical frameworks guiding leader interventions in each (Brown, 2010, 2023). Furthermore, clinicians who want to continue running groups after completing their graduate training have a responsibility to maintain their specialized group competencies by seeking consultation and supervision, staying up to date on the literature and practice guidelines, and furthering their training.
Well-trained group facilitators understand that group psychotherapy is a unique form of treatment that is equivalent in effectiveness to other types of psychotherapy. This understanding can be fostered by the study and use of evidence-based practice in group psychotherapy, as well as an understanding of therapeutic factors unique to groups (Barlow, 2013). However, while it is essential to be informed about and utilize the vast group psychotherapy literature, group competence also requires being able to assess how evidence-based practice and best practice recommendations may in part be a product of their social and historical contexts, therefore needing to be challenged or adapted to respond to the unique needs and experiences of diverse identities. In fact, group leaders should look at such evidence through a multicultural and social justice lens and be able to identify how dominant systems (e.g., White supremacist ideology, heteronormativity, ableism, etc.) have impacted the development of our field (Liu et al., 2019; Ribeiro, 2020). Frameworks such as liberation psychology and decolonization should be integrated into therapists’ training to allow them to provide the best care possible to all clients (Comas-Díaz & Rivera, 2020; Goodman et al., 2015).
Understanding the role of the group therapist is important to grasp why specialized training is necessary to run successful groups. Group leaders must conceptualize cases at the individual level, as well as the group level. In fact, while understanding the individual client and their presenting concerns remains an essential therapy skill for group leaders, they must also assess how those presenting concerns will fit in the group, as well as how each individual client might impact the group and its process. Barlow (2013) argues that group leaders must find the right balance between individual and group conceptualization and responding to individual needs and group needs. Balancing the use of interventions at group and individual levels is no small task requiring not only knowledge of overall psychopathology and interpersonal factors, but an understanding of group dynamics and group cohesion.
Specialized group competencies are not only essential to create and conduct successful therapy groups, but also to dispel stigma surrounding group as a valid form of treatment. Well trained group facilitators can advocate for clients to receive appropriate care, educate peers and colleagues, and create positive group experiences for those who might be hesitant to join.
The Group Setting
The first factor to consider when planning to create a new group is the setting in which the group will be held. The literature has described the creation of a new group as a complex process that not only involves the carefully assessed selection of clients who will participate in it (MacNair-Semands & Whittingham, 2023), but also consideration of the context surrounding the group (Bernard, et al., 2008; Yalom & Leszcz, 2020), including the referral sources of mental health and medical professionals, the setting in which the group is embedded, and insurance companies or other third-party payers (Yalom & Leszcz, 2020). As such, the creation of a successful therapy group requires willingness to and understanding of how to collaborate with these interfacing systems.
These contextual factors impact the viability of a new group in two main ways. First, the immediate environment in which the group is embedded, whether it be a clinic, hospital, community health center, and administrators of those settings, often dictate forms in which care can be provided and influence availability of resources (e.g., available rooms, financial resources, training opportunities, etc.). As such, therapists working in those settings should foster collaborative relationships with administrative staff. To do so, they can educate themselves about factors and challenges involved in securing and allocating resources, attend organizational meetings, and provide education about group psychotherapy to enhance the likelihood of referrals (Bernard et al., 2008). When working with insurers or third-party payers that determine what portions of treatment are paid for or, at times, length of treatment, group therapists can be advocates for increased accessibility to care by providing education about the benefits and outcomes of group psychotherapy (Bernard et al., 2008). Further, group therapists should be aware of the ways oppression (current and past) may manifest within the settings in which they practice in order to understand how potential clients may engage with their groups (Ribeiro, 2020). A successful group is one that creates a setting that makes space for understanding the marginalization of its members, in and outside of the therapeutic setting.
Other influences on the viability of a group are through soliciting appropriate referrals. The original AGPA Group Psychotherapy Practice Guidelines noted that “suitable referrals are the life source of the group” (Bernard et al., 2008, p.8). As new groups tend to have higher rates of attrition, good referrals are essential to sustain them (Rutan et al., 2020a). Unfortunately, many clinicians, administrators, and other individuals involved in decisions regarding clients’ care still lack knowledge of the efficacy of group therapy or training in running groups. This lack of knowledge and training, paired at times with stigma regarding group therapy as a less valid form of treatment (Yalom & Leszcz, 2020) can cause hesitation to refer clients to group. As a result, therapists should expect to provide some education and training to create a strong referral network and receive proper referrals.
Referrals and Marketing
Receiving client referrals that are an appropriate fit is essential for a group to be able to meet its goals and function properly. Therefore, when working with referral sources, group facilitators must provide clear information regarding the group’s goals, structure, expected composition, and process. The more information referral sources possess about a group’s goals and processes, the more likely the group will be successful (Rutan et al., 2020a). Lack of training may limit the clinicians’ ability to communicate how group could be helpful both to potential clients and referral sources who might hold negative biases about group therapy (Kaplan, 2017; Rutan et al., 2020a). The American Group Psychotherapy Association (AGPA) provides valuable training materials, such as these practice guidelines and the Group Therapy Training and Practice Series, that can be utilized to broaden training in the field (Brabender & MacNair-Semands, 2022; Joyce & Marmarosh, 2023; MacNair-Semands & Whittingham, 2023).
Education about the specific group that the therapist is planning to run is just as important as providing general education about group psychotherapy. When marketing groups to colleagues, administrators, or potential clients, therapists should make their materials as clear as possible regarding fit (inclusion and exclusion criteria), the group structure, fees, the goals of the group, what is involved in meeting those goals (e.g., group process), and all logistical aspects of the group (Bernard et al., 2008; Rutan et al., 2020a; Yalom & Leszcz, 2020). There are many ways to successfully market groups to clients, colleagues, and agencies. For instance, when marketing to clients, therapists should consider providing written materials about the group to help potential clients retain needed information (Bernard et al., 2008; Brabender & MacNair-Semands, 2022; Joyce & Marmarosh, 2023). Although much of the referral process occurs through already established connections between therapists, their colleagues, and other agencies, social media is now widely used by mental health professionals to advertise their work. Yalom and Leszcz (2020) highlight that marketing is about more than self-advertising. The tools available today can be used to build a stronger clinical practice, as well as to further educate the public and contribute to destigmatizing group psychotherapy. For therapists working in private practice, the majority of marketing and education will be their responsibility. Therapists working in agencies, however, may consider creating group coordinator positions to navigate those issues.
Type of Group and Therapeutic Goals
Since one of the group leader’s primary responsibilities is to create and implement group norms in a therapy group (Rutan, et al., 2020b), it is essential for group therapists to have a clear vision of the type of outcomes they hope to see in clients participating in their group. Turner (2017) and Ribeiro (2020) put forth that therapists can promote group cohesion by defining group expectations and rules and guiding members in their participation. To achieve this goal, therapists should first define the type of group they want to run. There are many forms of group therapies with different goals and processes, often related to therapists’ theoretical orientation and clients’ presenting concerns. For instance, an interpersonal group’s goals are to allow interpersonal processes to emerge in the group in order to utilize interpersonal experiences to change them through insight and feedback, or corrective emotional experiences (Mahon and Leszcz, 2017). These types of groups approach the group as a social microcosm (Yalom & Leszcz, 2020), utilize the here-and-now to guide the process, and are less structured than other types of groups. In contrast, cognitive behavioral groups (CBT groups) are more likely to be structured and time limited. Such groups aim for symptom reduction and use specific interventions to address symptoms in and out of session. Extensive research on CBT makes those groups more likely to be used in agencies and treatment centers, or for specific symptomatic presentations such as anxiety. It is important to note that there are many types of groups offering various options for therapists and clients (e.g., Dialectical Behavioral Therapy Groups, humanistic and existential groups, mindfulness-based group, compassion-focused groups, or psychoeducational groups, etc.). Therapists often guide their choice of group based on their own clinical preference, the settings in which they work, and the populations they see. Many contemporary group leaders integrate aspects of different group theories to their practice (Kaklauskas & Olson, 2020). However, it remains important to identify what is expected for a specific group before the group starts as it will allow group therapists to formulate specific goals, structure their approach in the group, and communicate its goals to others (e.g., referral sources).
Needs Assessment
Once group leaders know the type and aims of the group they want to run, they can assess whether the group will be a good fit for the settings in which they work. Rutan et al. (2020a) identify two factors to consider before creating a therapy group: need and feasibility. First, to optimize the success of their group, therapists should determine if there is an actual need for the type of group they want to run in the setting in which they practice. Although a group might seem like a good idea or fit within a therapist’s area of expertise and clinical interest, lack of need for it will impact client recruitment, administrative buy in, and, ultimately, the viability of the group. In addition to need, considering feasibility is also important. For example, group therapists should ask themselves if the group is a good fit for the setting in which it will be held (e.g., running a long-term process-oriented group in a short-term treatment facility), if its goals and values fit within the goals and values of the agency where it will be run, or if there will be enough incoming referrals to sustain it (Rutan et al., 2020a). These questions are particularly relevant for the therapists who work in institutions such as hospitals or treatment centers, which might impose more structure and time limits to the type of care that can be provided.
Group Structure
In addition to setting goals and expectations for the group, another group therapist responsibility is to set the group’s structure and communicate it clearly to referral sources and potential clients.
Time and place: Group leaders decide when and where a group will meet. It is their responsibility to maintain consistency in location and start and end times. Consistency is essential when running therapy groups, as coordinating multiple different schedules can be especially difficult. Group therapists often have to consider running groups at times that fall outside of the typical workday to accommodate as many potential group members as possible. Any change in the group schedule after the group has started should be discussed with the group ahead of time (Rutan et al., 2020a).
Session frequency and duration: While research on group sessions’ frequency and length is limited (Rutan et al., 2020a), Yalom and Leszsz (2020) note that the first 60 minutes of a group session allow for the main themes to emerge, indicating that group sessions need to last longer than a typical 50-minute individual therapy session. However, they recommend not exceeding two hours, as both the group’s and the therapist’s effectiveness seem to diminish after that. Although this might be impacted by the setting in which the group is held (e.g., community mental health center vs. private practice), group sessions lasting about 90 minutes appear to be the consensus among experienced group therapists and in the literature (Yalom & Leszcz, 2020).
Yalom and Leszcz (2020) also indicate that weekly group therapy sessions tend to contribute to “greater therapeutic connection” (p.346), while less and more frequent sessions do not necessarily appear to be beneficial. As with other decisions related to the structure of the group, some clinical settings, and even some treatment protocols (e.g., DBT groups) have specific expectations regarding session duration and frequency. While a therapist in private practice will have much more flexibility in terms of scheduling, therapists working in institutions or taking specific insurances might have to comply with different rules and expectations regarding duration of session and frequency. Although those limitations might not always be in the best interest of the clients, therapists might need to navigate such systems to continue offering care. Ideally, decisions regarding session length and frequency should be informed by therapist’s theoretical orientation and group goals (Rutan et al., 2020a).
Group size: Group size may vary based on the type of group. For instance, psychoeducational groups tend to be larger than process-oriented groups. Group size may also be impacted by space available and institutional policies. For instance, some agencies may not allow groups to begin until a specific number of members is enrolled and consistently attending (Rutan et al., 2020a). Regardless of agency policies and resources, the group literature has emphasized that group size has an impact on the group process. When deciding how many members to include in a group, therapists should be aware that smaller groups (four and below) tend to become more passive with less member-to-member interactions and more individual therapy-like work. On the other hand, larger groups can make it difficult for members to have enough time to work through individual concerns, which could impact cohesion. The consensus, according to the literature, is that seven or eight member groups tend to work best (Burlingame, et al., 2013; Yalom & Leszcz, 2020). To counter attrition, group facilitators may choose to start a group with a higher number of members than they hope to have.
The composition of the group is another factor requiring therapists’ thoughtfulness and preparation and is addressed in Chapter 3: Selection of Clients and Group Composition.
Open versus closed group: Another important decision that group leaders must make before a group starts is whether the group will be open or closed. A closed group is a group that will not accept new members once it has started, whereas an open group will continue accepting new members. When making this decision, therapists should take potential dropouts and group size into account. Closed groups tend to be time-limited and briefer and should start with a higher number of members (9-10) to counter attrition (Yalom & Leszcz, 2020). They also appear to be a better fit for groups following a specific curriculum (Rutan et al., 2020a). Open groups work in a variety of settings, including where clients are likely to be long-term members of the group (e.g., incarcerated populations). When leading an open group, group leaders should pay special attention to the way the group adjusts to new members and the way new members integrate into the group, including processes of accommodation and assimilation, respectively (Rutan et al., 2020b).
Space and accessibility: When creating a group, therapists’ decisions will be impacted by the space in which the group will be held. For instance, group size might be dependent on the size of rooms available to clinicians. Groups should be held in spaces that guarantee privacy and that are low in distractions. In some settings, therapists will have to advocate to have access to such spaces for their groups (Yalom & Leszcz, 2020). Therapy spaces should also be accessible to all potential clients. For instance, therapists should hold groups in spaces that are accessible to clients with diverse mobility needs or that include chairs comfortable for all bodies. Therapists can also consider office spaces that are accessible by public transportation. Therapy spaces should be welcoming to individuals from diverse identity backgrounds and accessibility needs.
Group Norms and Agreements
Before meeting potential group members, group therapists should have an idea of what norms will be important to guide members in their group participation and facilitate the formation of group cohesion. The goal of the group norms is to help maintain the safety of the group and ensure that the group can appropriately be a container of what members experience in it. The norms will be discussed and adjusted with individual clients during the preparation meeting (also see Chapter 4) and with the group when the sessions begin. Some group therapists develop a group agreement signed by members to introduce the norms and help set clear expectations for the group. In general, we recommend that group agreements include information such as (Rutan et al., 2020a):
- Confidentiality and how it will be protected. This should also address the members’ responsibility to protect each other’s privacy and information.
- Discussion of dual relationships and contact outside of group.
- The group goals and a commitment to them.
- Expectations regarding the role of members in the group process and the role of the therapist(s). This would include information specific to the theoretical framework adopted by the therapists leading the group.
- Information regarding group boundaries, inappropriate behaviors, and how boundary violations will be addressed and managed.
- How to manage termination or leaving the group.
- Information about fees and ways to pay them.
Co-leadership
Co-leadership refers to the collaborative relationship between two group facilitators leading a group together. Although co-leading a group has many benefits for therapists and group members, it is also important to recognize that it adds to the already existing complexity of group therapy (Greene, et al., 2020). As such, this leadership decision can have a significant influence on the success of a therapy group. Unfortunately, there is limited literature on group co-leadership to guide therapists trying to decide whether to lead a group solo or with a co-leader, and much of this decision appears to rely on therapists’ personal preference (Greene et al., 2020; Kivlighan, et al., 2012).
The Practice Guidelines for Group Treatment in the Netherlands emphasize the importance of preparation in creating a long-lasting successful co-leadership. The authors suggest having conversations before the beginning of group regarding the goals and approach to take in the group. They also recommend that these conversations address each therapists’ theoretical orientation or preference, training and experience, personal motivations for running the group, personal needs, and the logistics involved in running the group (Huffstadt & Remijsen, 2019). Before the group begins, co-leaders should discuss expectations for the group and each other, as well as how they will support each other throughout the course of the group. Furthermore, co-leaders may differ in identities and may benefit from discussing these differences. Many authors are now also expressing the need for more information around how cultural insensitivity in clinical encounters might be experienced or predicted by members, particularly by those who have experienced racism or discrimination (Kaklauskas & Nettles, 2020; Ribeiro et al., 2017; Yalom & Leszcz, 2020). Those concerns and plans on how to address them in the group must be discussed before the group begins. Throughout the length of the group, preparation, processing, and planning between sessions should continue to ensure that co-leaders stay on the same page (Greene et al. 2020).
Summary
Much of what goes into creating a successful therapy group occurs before the group begins meeting. Group therapists can set their groups up for success by:
- Understanding the settings and contexts in which they practice, particularly the resources they offer and constraints they impose;
- Educating their professional community and the general public about the benefits of group psychotherapy and responding to explicit or implied negative biases and resistances to group therapy;
- Developing clear goals for their group;
- Identifying a clear group structure and well-defined work roles that fit the purposes for which the group is created (i.e., form should follow function);
- Communicating clear information about their group to potential clients and referral sources and addressing concerns or biases;
- Understanding what is needed for effective leadership in this specific group.
Therapeutic Processes
Clinical experience and research demonstrate that group psychotherapy is effective across a wide variety of human challenges. In fact, a strong body of outcome research shows that group psychotherapy is an effective form of psychotherapy across diagnoses, clinical populations, and treatment settings (Burlingame & Strauss, 2021; Burlingame, et al., 2016; Yalom & Leszcz, 2020). However, the “how” and the “why” of group psychotherapy effectiveness are not as easy to understand or to assess as its outcomes. Some of the earliest writings on group psychotherapy suggested that the “fine spirit of camaraderie” between members provided unique support, encouragement, and re-education, (Pratt, 1907, p.756). Over the last several decades, these subtle processes that lead to positive outcomes have been labeled as therapeutic factors, process variables, and change mechanisms. Awareness of therapeutic factors allows the group leader to see below the surface-level content of discussions and into the depth of potentially healing moments in the psychotherapy group.
Historically, group therapeutic factors have been presented and utilized from a Eurocentric modernist perspective, and rightfully critiqued from critical theory traditions, postmodern, queer, social justice, and other lenses as being biased and potentially not fitting for all members and all groups. Group psychotherapy is moving toward a more ideographic frame and with this shift comes exciting and creative opportunities for group leaders. Each group, group member, and leader are embedded within unique cultural contexts, and drawing solely on the historical theories and research that are grounded in dominant cultural perspectives and identities is limited, and potentially misguided. Leaders need to continually educate themselves on the traditional and contemporary healing processes of the group members and their communities, as well as their current context. While scholarly learning is important, collaboration with individual members and systems is vital to skillfully expand and broaden the range of therapeutic interventions. Depending on the setting, goals of the group, and group members’ identities, a leader should be flexible to effectively respond to the unique needs of the diverse group members (Kaklauskas & Nettles, 2020). As discussed throughout the guidelines, group leaders’ multicultural competence should go beyond simple flexibility. As group leaders, we must be ready to examine our own positionality, power, privilege, and cultural identities and how they might impact group dynamics and alliance.
While the discussion below provides the historical theory and contemporary research findings, group practice is not static and needs to be modified and adjusted to meet the moment with the members. The section aims to provide some background from which leaders can build toward what will be most impactful in their own groups.
Therapeutic Factors
Following World War II, group psychotherapy experienced an expansion to meet the demands for services. From the dominant cultures of Europe and the United States, many enduring group psychotherapy ideas were introduced concerning group development, group structure, and group-as–a-whole dynamics. Alexander’s and French’s (1946) conception of “corrective emotional experiences” became a building block for understanding the healing movements in therapy and also began to be widely applied to psychotherapy groups. Alexander and French stated, “the patient, in order to be helped, must undergo a corrective emotional experience suitable to repair the traumatic influence of previous experiences” (p. 66). Groups can provide unique interchanges that can move members toward healing by having disconfirming and new experiences that allow members to feel, think, and behave in new ways.
Drawing on the work of previous researchers, the most well-known taxonomy of group change mechanism, or therapeutic factors, comes from Yalom and Leszcz (2020).
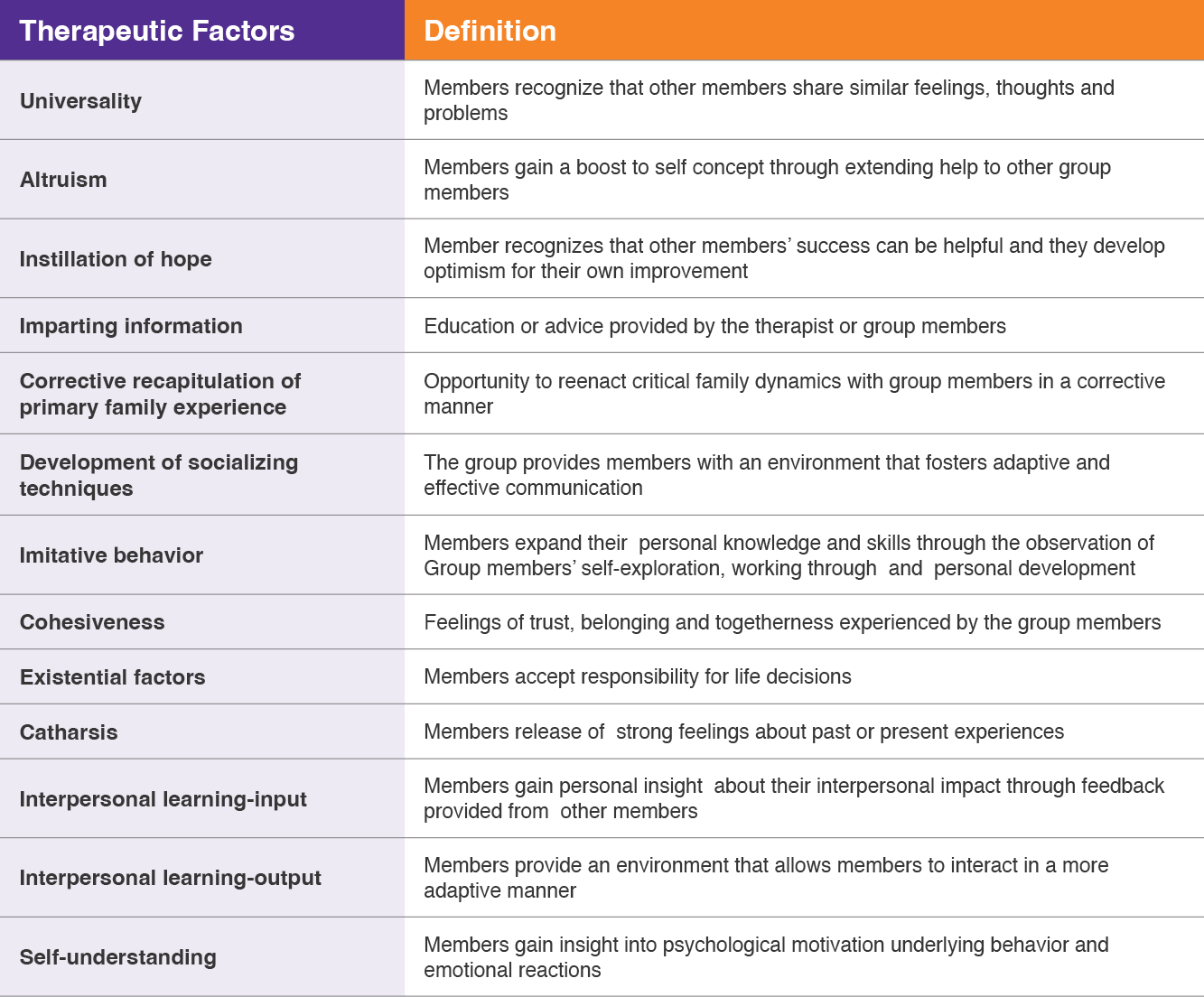
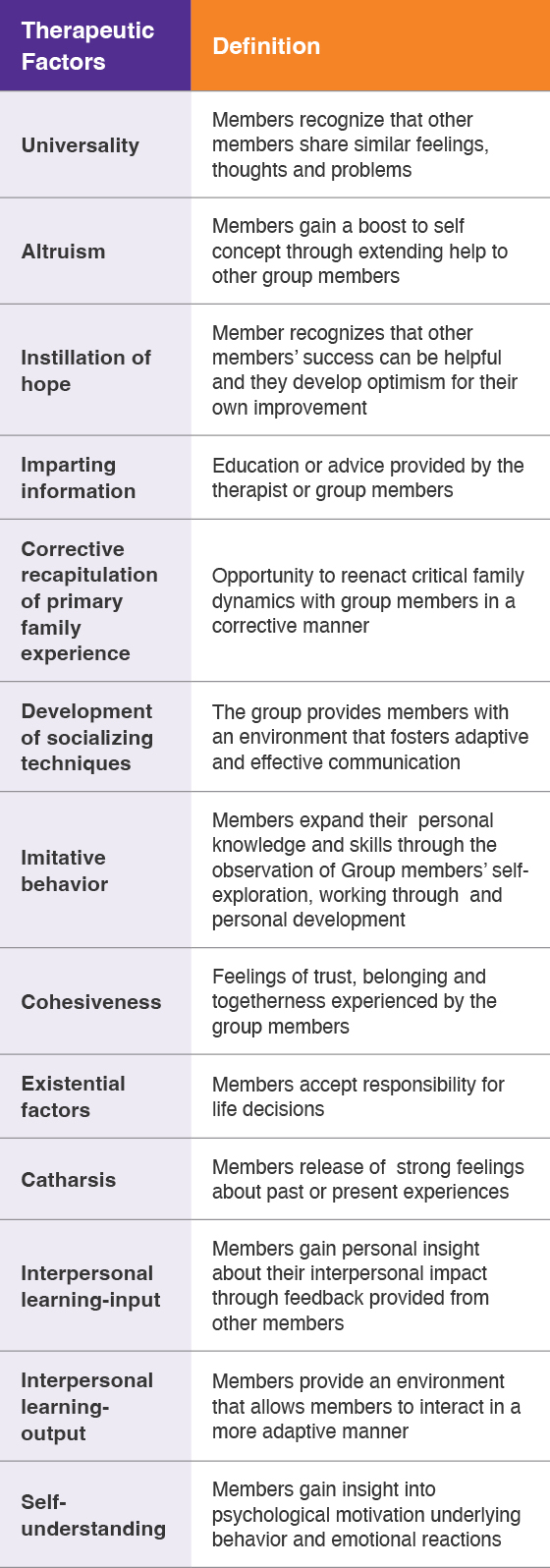
Table 1
Therapeutic Factors (Yalom and Leszcz, 2020)
|
Name of Therapeutic Factors |
Definition |
|
Universality |
Members feel supported and understood by recognizing that other members share similar feelings, thoughts, and challenges that can lessen feelings of isolation. |
|
Altruism |
Members engage in meaningful experiences by extending help to other group members. This can expand the self-concept and create mutuality in outside relationships. |
|
Instillation of Hope |
Members experience encouragement and support and observe other members’ successes. Situations that may feel difficult or long-lasting may be seen from a new perspective with potential positive changes. |
|
Imparting Information |
New knowledge, ideas, coping skills, and/or advice are provided by the therapist or other group members. |
|
Corrective Recapitulation of Primary Family Experience |
The opportunity to reenact critical family dynamics with group members in a corrective manner. |
|
Development of Socializing Techniques |
The group provides members with an environment that fosters experiencing and practicing new flexible, adaptive, and effective relational and communication patterns. |
|
Imitative Behavior |
Members expand their personal, relational, communication, and behavioral repertoire through the observation of other members and group interactions. |
|
Cohesiveness |
Feelings of trust, belonging, and togetherness experienced by the group members. The feeling that the group is working together for the benefit of all members. |
|
Existential Factors |
Members consider existential factors including limitedness, choice, and responsibility for life decisions. |
|
Catharsis |
Members release strong feelings about past or present experiences. This emotional discharge can sometimes lead to new insights. |
|
Interpersonal Learning—Input |
Members gain personal insight about their interpersonal impact through feedback provided from other members. |
|
Interpersonal Learning—Output |
The group provides an environment that allows members to explore and practice new self and relational patterns. |
|
Self- Understanding |
Members gain insight into psychological and historical reasons motivating underlying behavior and emotional reactions. |
These factors are likely to operate in most types of groups, but depending on the goals of the group, some may be more saliant than others. D. M. Jr. Kivlighan et al. (2004) suggested a four-category typology of groups in which different factors may be highlighted, based on the same:
- Affective support groups that may include grief or trauma-oriented groups that place emphasis on the factors of installation of hope, universality, cohesion, and acceptance.
- Affective insight groups, such as psychodynamic and personal growth process groups, prioritize catharsis, interpersonal learning, and self-understanding.
- Cognitive insight groups, such as cognitive-behavioral groups, may accentuate interpersonal learning output, self-understanding, and imitative behavior.
- Cognitive support groups, which may include recovery and relapse prevention, often focus on vicarious learning and guidance.
Specific or technical therapeutic factors can be linked to theoretical orientations and specific views of change processes (Greene et al., 2020), as exemplified by:
- Practicing mindfulness in groups in Dialectical Behavioral Therapy groups.
- Evaluating one’s values in Acceptance and Commitment Therapy groups.
- Role playing a situation in psychodrama.
- Exploring transference in psychodynamic groups.
As leaders, we can try focusing our attention towards the therapeutic factors that best fit the context, our membership, and the group’s goals (D. M. Jr. Kivlighan et al., 2010). As cohesion continues to have most significant empirical support across all types of groups, most leaders begin by trying to foster a sense of belonging, teamwork, and shared missions, which may allow the group to work most effectively. While the emphasis of which therapeutic factor to focus upon depends on context, in addition to cohesion, many leaders also highlight social learning, emotional expression, hope, and understanding of one’s relational impact on others. In an attempt to simplify this topic, Tasca and colleagues (2016) tried to capture the current theory and research in one global process factor, “feeling hopeful about the processes of emotional expression and relational awareness, which then translate into and promotes social learning” (p. 140).
The Therapeutic Alliance
The quality of relationships in the room is also central to creating change in group settings. Ideally, group members develop a therapeutic alliance with the leader—a shared commitment to work on the therapeutic goals and tasks. This begins in the intake interview through the therapist’s demonstrating an understanding of their presenting concerns, cultural identity and experiences, their current situation, and being forthright about the processes and outcomes they may experience through group participation. Alliance can also be supported throughout the groups, from acting ethically and holding the group structure through expressions of empathy, therapeutic presence, and mirroring and reflecting upon what members have said (Alldredge et al., 2021). As leaders, if we strive to be consistent, dependable, aware of power dynamics in the group and our role in them, and faithful to our word, the alliance will continue to build over time. However, relational ruptures between leaders and members do occur. These need attention lest harm occur, but they also offer opportunities for building deeper understanding. As leaders, we may need to make shifts in our behaviors, as well as the group’s goals or group processes that would better serve the members.
While there are many types of ruptures, microaggression, invalidations, and other damaging socio-cultural events in group need to be addressed quickly to rebuild trust and prevent premature termination. The leader needs to understand the impact on the member without defensiveness or interpretation, and work to do better in facilitating culturally responsive ways (Kaklauskas, 2021). Also, a leader can build and maintain alliance through identifying and confronting other destructive group dynamics, such a scapegoating, avoidance of the group’s work, and boundary violations. Having members name and explore their social locations, the contextual obstacles, privileges in their lives, the impact of the socio-cultural bias, and the environment on their lives is essential in addressing the realities of members’ lives and promoting a sense of inclusiveness and awareness across identity differences between members (D. M. III. Kivlighan & Chapman 2018; Singh, et al., 2020).
Compared to individual therapy, alliance in group therapy is multilayered. In fact, group interactions happen at three levels: member-to-therapist, member-to-group, and member-to-member (Burlingame et al., 2013; Lo Coco et al., 2019). Therefore, positive bonds can occur at each of those levels. Besides the quality and depth of the therapeutic alliance with the therapist, the nature of the bonds and affective ties between and among the members is important in developing cohesion and a shared sense of the value of the group, its meaningfulness, and its purpose. As a result, members can be encouraged to empathically explore their relationships with one another by risking the sharing of more details about themselves and discovering and containing differences in their experiences and viewpoints.
Specific schools of psychotherapy and contemporary developments also suggest additional healing factors, such as:
- In attachment-based group work, finding techniques and interchanges that support empathic attunement, repairing relational ruptures, and exploring internalized models of self, others, and relationships may be central (Marmarosh & Magenheimer, 2018; Tasca & Maxwell, 2021).
- In mindfulness-based groups, practicing mindfulness exercises, expanding one’s awareness to the members internal and external stimuli, and focusing on regulation can lead the way. (Chang, et al. 2017).
- In creative art-based groups, such as art or music therapy, creating a space for free expression and playfulness are part of the therapeutic journey (Haen & Webb, 2019).
While the focus may be different depending on the group goals and the definition of work within each theoretical orientation, each of the above can be beneficial in most contemporary group treatments.
While acknowledging and building upon the significant previous work of therapists and theorists, therapeutic factors should be seen as always evolving. Being familiar with seminal ideas gives leaders a foundation to build upon and develop their own conceptualizations of those processes that lead to therapeutic change. Thinking about what is going on in the here-and-now of the group, with curiosity, hovering attention and desire to make meaning, is a never-ending task of the therapist. This analytic work is simply too complex for the therapist to believe they have a complete understanding of what is occurring and why. Even the most empirically reviewed and endorsed factor of cohesion needs to be seen not as an isolated and unitary variable but rather as a dimension in complex interaction with other factors, such as group composition (Burlingame, et al., 2018); there are times and situations, for example, where cohesion can be experienced as toxic or threatening to the need for separateness and individuation. As covered in the other areas of this text, many elements beyond therapeutic factors come together to affect outcome, including group structural arrangements (such as unstructured exploration versus directive interventions like assigning homework), cultural sensitivity and humility on the part of the therapist and the members, treatment dosage, ethical practice, and onwards.
Moreover, as Chen et al. (2008) and others advocate, the advancement of the field ultimately needs to bring together the classical perspective, such as the work on therapeutic factors with a multicultural viewpoint, domains that have historically been siloed. While the research is limited, evidence and clinical experience support this idea of integrating foundational knowledge, such as that pertaining to therapeutic factors, but with critical thought to contexts (e.g., race, class, disability, gender, etc.; Johnson & Lambie, 2013).
Of central importance is the leader’s and/or group members’ work on developing cultural humility and awareness. Dominant culture identified group therapists are more likely to seek the comfort of universality than the social learning of exploring differences (Belcher Platt, 2017). The need for cultural adaptions to existing models is clear, as often the behavioral choices, challenging situations, metaphors, and language described in certain theories or manualized treatments may not transfer to all the citizens of the world, let alone to any particular nation or region (Ziadeh, 2020). One approach does not fit best with every group, and leaders should modify or substitute new protocols to meet the composition and context of the membership of their groups. In this way, the cultural competence, sensitivity, and critical awareness of any group leader are perhaps the most important of all therapeutic factors.
As group psychotherapy expands globally and works towards collaboration with our diverse society, leaders have options to continue to develop new methods and group interactions for the benefit of their members. Members of marginalized demographic groups are less likely to attend psychotherapy; thus, leaders must improve in meeting their members in the moment. Many leaders are incorporating culturally specific practices into their group work, such as music, dance, and other rituals. While the adaptation of previous models into new contexts continues, some practitioners and theorists are developing group therapy approaches born from specific cultures as opposed to using older models in every situation (Lyn, 2022). In this way, group psychotherapy and therapeutic factors theory is engaged in a transformative process. Corrective emotional experience may look different from varied socio-cultural perspective and experiences.
Leaders should collaborate with their members to foster dialogue that invites the most applicable of the old, while simultaneously looking forward to meeting the various needs in diverse contexts. With careful, critical thought utilizing therapeutic factors in our groups, we can benefit our members personally, and potentially contribute to building alliances and bonding throughout our society.
Summary
- Understanding therapeutic factors and mechanisms can help group therapists conceptualize their groups and understand the processes at play.
- Monitoring what is occurring in the moment in the group—therapeutic processes as well as nontherapeutic processes—is complex work requiring ongoing curiosity, hovering attention, and a desire to make meaning. This can also be done using assessments.
- Historically, therapeutic factors have been studied from a Eurocentric lens. The field now understands that this lens needs to be widened to include and integrate multicultural and social justice-oriented perspectives to meet the needs of all clients.
Table 1. The Therapeutic Factors (Yalom and Leszcz, 2005)
Specifically, the distinctiveness of some client characteristics, therapeutic interventions and therapeutic factors (examples include insight, catharsis, hope, reality testing) was not found when comparing major empirical reviews of the individual and group literature. On the other hand, distinctive mechanisms of action emerged when multi-person relationship factors were considered. Participating in a therapeutic venue comprised of multiple therapeutic relationships produced therapeutic factors that were unique to the group format (examples include vicarious learning, role flexibility, universality, altruism, interpersonal learning). Empirical support for this proposition followed in a study (Holmes & Kivlighan, 2000) that found participants reported higher levels of relationship, climate, and other-focused processes as responsible for change in group when contrasted with clients participating in individual treatment.
Cohesion — a core mechanism of action. Of the described therapeutic factors (TFs), we consider the mechanism of cohesion to be most central — it is a therapeutic mechanism in its own and it facilitates the action of other TFs. There is growing consensus that cohesion is the best definition of the therapeutic relationship in group (Burlingame et al., 2002; Yalom & Leszcz, 2005). In general, the therapeutic relationship is the ubiquitous mechanism of action that operates across all therapies (Martin et al., 2000). It appears as important, if not more important, in explaining client improvement than the specific theoretical orientation practiced by the therapist (Norcross & Goldfried, 2001). Indeed, in an extensive review, Wampold (2001) argued that common factors such as the therapeutic relationship may account for up to nine times greater impact on patient improvement than the specific mechanisms of action found in formal treatment protocols.
Cohesion defines the therapeutic relationship in group as comprising multiple alliances (member-to-member, member-to-group, and member-to-leader) that can be observed from three structural perspectives — intra-personal, intra-group, and interpersonal (cf. Burlingame, et al., 2002). Intrapersonal cohesion interventions focus on members’ sense of belonging, acceptance, commitment, and allegiance to their group (Bloch & Crouch, 1985; Yalom and Leszcz 2005) and have been directly related to client improvement. For instance, members who report higher levels of relatedness, acceptance, and support also report more symptomatic improvement (Mackenzie & Tschuschke, 1993). Intra-group definitions of cohesion focus on the group-level features such as attractiveness and compatibility felt by group-as-a-whole, mutual liking/trust, support, caring and commitment to “work” as a group. This definition of cohesion has been linked to decreases in premature dropout (Mackenzie, 1987) and increased tenure (Yalom and Leszcz, 2005). Finally, interpersonal definitions of cohesion focus on positive and engaging behavioral exchanges between members and have been linked to symptomatic improvement, especially if present in the early phases of group sessions (Budman et al., 1989).
Relation of cohesion to other therapeutic factors. Cohesion has shown a linear and positive relationship with clinical improvement in nearly every published scientific report (Tschuschke and Dies, 1994). Beyond this evidentiary base, it has also been linked to other important therapeutic processes. High levels of cohesion have been related to higher self-disclosure which leads to more frequent and intense feedback (Fuehrer & Keys, 1988; Tschuschke & Dies, 1994). A positive relationship between cohesion and self-disclosure, member-to-member feedback, and member-perceived support/caring has also been demonstrated (Braaten 1990). In addition, early and high levels of engagement may buffer group members from becoming discouraged or alienated when subsequent conflict takes place during the “work” phases of the group (MacKenzie, 1994; Castonguay et al., 1996). Notwithstanding the promising relations between cohesion and other important therapeutic factors, it must be acknowledged that most studies were correlational, making it difficult to determine causality.
The number of articles, chapters, and books about cohesion and its relationship to successful groups is so large (MacKenzie, 1987; Colijn et al., 1991) that attempts to derive evidence-based principles for its development and maintenance often seem daunting. Table 2 offers a summary of a recent review of well-researched group dimensions that have been empirically linked to cohesion: group structure, verbal interaction, and emotional climate.
Table 2 Evidence-based Principles Related to Cohesion (Burlingame et al 2002)
Use of Group Structure
Principle One. Conduct pre-group preparation that sets treatment expectations, defines group rules, and instructs members in appropriate roles and skills needed for effective group participation and group cohesion.
Principle Two. The group leader should establish clarity regarding group processes in early sessions since higher levels of early structure are predictive of higher levels of disclosure and cohesion later in the group.
Principle Three. Composition requires clinical judgment to balance intrapersonal (individual member) and intragroup (amongst group members) considerations.
Verbal Interaction
Principle Four. The leader modeling real-time observations, guiding effective interpersonal feedback, and maintaining a moderate level of control and affiliation may positively impact cohesion.
Principle Five. The timing and delivery of feedback should be pivotal considerations for leaders as they facilitate the relationship-building process. These important considerations include the developmental stage of the group (for example challenging feedback is better received after the group has developed cohesiveness) and the differential readiness of individual members to receive feedback (members feel a sense of acceptance).
Establishing and Maintaining an Emotional Climate
Principle Six. The group leader’s presence not only affects the relationship with individual members but all group members as they vicariously experience the leader’s manner of relating. Thus, the leader’s management of his or her own emotional presence in the service of others is critically important. For instance, a leader who handles interpersonal conflict effectively can provide a powerful positive model for the group-as-a-whole.
Principle Seven. A primary focus of the group leader should be on facilitating group members’ emotional expression, the responsiveness of others to that expression, and the shared meaning derived from such expression.
These dimensions reflect classes of interventions that have direct implications for clinical practice. More specifically, group structure reflects interventions (e.g., pre-group role preparation, in-group exercises, and composition) designed to create specific member expectations or skills used in the group or group operations, including the establishment of group norms. Verbal interaction reflects global principles of how a leader may want to model or facilitate member-to-member exchange over the course of the group. Emotional climate reflects interventions aimed at the entire group experience, with the aims of increasing safety and the work environment of the group. Some of these dimensions are discussed herein and throughout this document, while others are better understood by consulting the original source of Table 2 (Burlingame et al., 2002).
Assessment of therapeutic mechanisms in clinical practice. For those clinicians who have an interest in tracking the therapeutic relationship in group psychotherapy, the American Group Psychotherapy Association (Burlingame et al., 2006) recently released a Core Battery of instruments to assist group clinicians in selecting members, tracking their individual improvement, and assessing aspects of the therapeutic relationship. This task force relied upon a recent study that sought to simplify the underlying dimensions used to describe the therapeutic relationship in group and evaluate the group process (Johnson et al., 2005). Taken together, the measures address three components of the group therapy experience: the positive relational bond, the positive working relationship, and negative factors that interfere with the bond or the work of therapy. In addition, each component is addressed in terms of two perspectives: the member’s relationship with the therapist and the member’s relationship with the group as a whole. Table 3 indicates how each measure (or subscale of a measure) can be used to evaluate each of the six possible component-perspective combinations.
Table 3 CORE Battery Process Measures (Burlingame et al., 2005)
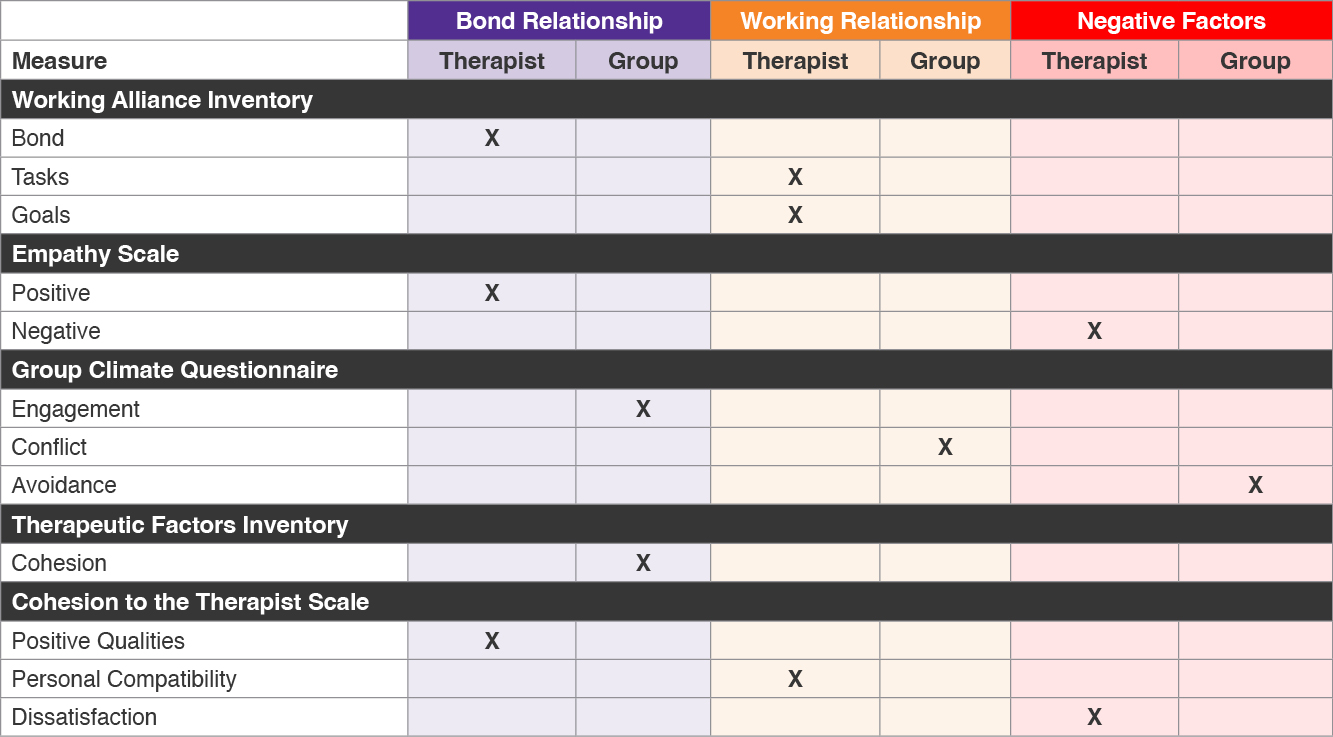
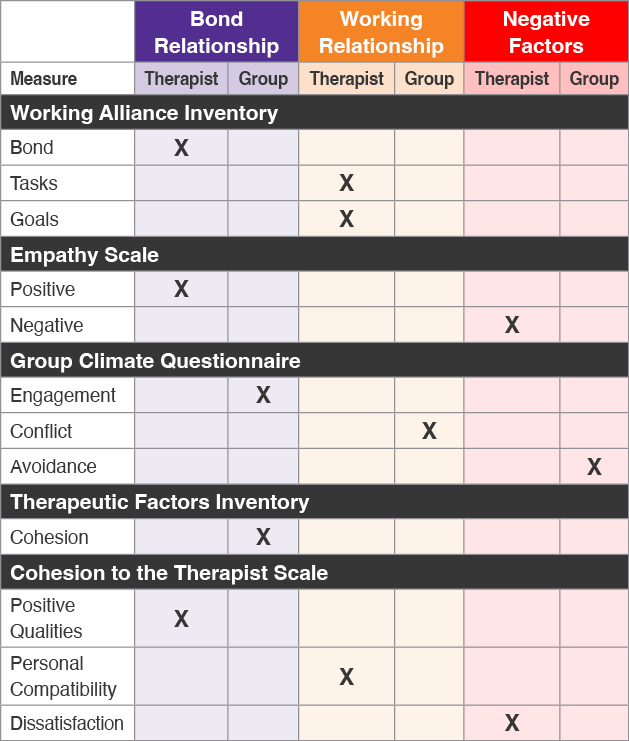
A critical and unique therapeutic mechanism of change in small group treatment relates to the interpersonal environment, often referred to as the social microcosm created when the leader and members join together in a therapeutic collective. In addition to the therapist’s clinical sense, empirical assessment tools provide a structured approach to “taking the pulse” of the group interpersonal climate to ascertain what may be obstructing or facilitating interpersonal processes at a group level. Leaders play a pivotal role in modeling and shaping this interpersonal environment (Fuhriman & Barlow, 1983) and are advised to pay careful attention to these particular mechanisms of change. It is particularly wise to focus upon the relational bond, working relationship/therapeutic alliance, and negative factors. Attention to these elements underscores the possibility that ruptures in the leader-member relationship may occur which can impede the work of therapy for a member or at times for the group as a whole, and even lead to the premature termination of members. Therapeutic interventions intentionally targeting different structural units of the group (member-to-member, member-to-group, and member-to-leader) are encouraged as the therapist creates and/or maintains specific mechanisms of change.
Summary
- The group psychotherapy literature underscores the importance of leaders having an understanding of mechanisms of change that are unique to group treatment (i.e. therapeutic factors) so that group-level interventions are guided by theory and empirical evidence.
- Developing and maintaining a healthy group climate involves the therapist monitoring and intervening at three structural levels of the group: intra-personal, intra-group, and interpersonal.
- Group leaders can employ three classes of group-level interventions — structure, verbal interaction, and emotional climate— at strategic developmental stages of the group to develop and maintain a health group climate.
- AGPA has developed the CORE BATTERY-R, (Burlingame et al., 2006) a set of evidence-based measures to assist group leaders in monitoring the therapeutic climate of their groups and their clients’ progress with the aim of increasing the overall effectiveness of group psychotherapy.
Client Selection and Group Composition
As Kealy and colleagues (2016) posit, client selection and group composition go hand in hand. That is, in assessing a potential group member, the therapist needs to maintain a dual focus, exploring both the suitability, readiness, and fit of a particular client for a particular group (either an established group or one that the therapist has in mind), and the resulting viability and functionality of the group. Both foci—member and group—need to be thoughtfully considered. On one hand, the therapist needs to explore the extent to which this particular patient will benefit from participation in this particular group by assimilating into the group, committing to its defined task and work, and valuing the enterprise. On the other hand, the therapist needs to imagine how an existing group will accommodate to the introduction of a new member or how the “blend of clients” (Brabender & MacNair-Semands, 2022) in a newly forming group will congeal and cohere to become a therapeutic working environment for all of its members (Bernard et al., 2008; Joyce & Marmarosh, 2023).
Client selection thus is informed both by an exploration of the potential member’s psychological resources—including capacities for empathy, reflection, access to one’s internal world, and interpersonal style that are likely to be manifest in the group—and by the goals of the group and the work required to reach those goals. Optimally, selection decisions positively affect the prospective member and the group in terms of therapeutic benefits. The selection process is, indeed, complex, and there is always the potential that therapists can get it wrong, that their decisions can be problematic or antitherapeutic for the individual prospective member, as well as the group-as-a-whole (Kealy et al., 2016). In fact, Kealy and colleagues’ work (2016) suggests that a group leader’s awareness that selection errors are likely to happen can help them engage in the selection process with more intentionality. Furthermore, they posit that therapists who are willing to accept that selection errors will happen can be prepared to implement reparative interventions upon realizing that there is a mismatch between the client and the group.
Because it involves many intersecting variables, client selection is a complex process that cannot be simplified through the application of specific instructions. However, understanding what typically makes clients successful, or not, in group therapy can help group facilitators make informed decisions or educated hypotheses about who to include in their groups. The primary consideration in client selection is whether an individual will be able to engage in the primary tasks and work of the group. A client’s ability to do so is impacted by their presenting concerns and their psychological makeup, including expectations of what group participation will be like and their motivation to do the work of the group, whether it be exploring interpersonal relations in the here-and-now or learning about how to cope with symptoms (Joyce & Marmarosh, 2023). Inclusion and exclusion criteria have emerged from the group psychotherapy literature to guide group facilitators in selection clients for group.
Inclusion Criteria
First and foremost, clients are a good fit for a group when their goals align with those of the group, such as improving coping skills or gaining insights into one’s relationships with others (Bernard et al., 2008; Brabender & MacNair-Semands, 2022; Rutan et al., 2020; Yalom & Leszcz, 2020). Therefore, inclusion criteria may vary by type of group (Joyce & Marmarosh, 2023). While following common inclusion criteria is helpful, therapists should also use their clinical judgment when making decisions about client inclusion into a specific group (Brabender & MacNair-Semands, 2022; Yalom & Leszcz, 2020). Brabender & MacNair-Semands (2022) state that not meeting inclusion criteria might not always indicate that someone will not benefit from group and that therapists’ insight into a client’s presentation is important in making selection decisions. False negatives (i.e., bringing someone into the group who might not meet the inclusion criteria but who actually participates in the work of the group) is much less problematic than false positives (having a prospective member who meets the inclusion criteria join the group but then turns out not to be committed to the task and work of the group).
Motivation
Yalom and Leszcz (2020) posit that a client’s motivation for change, as well as for achieving the goals and collaborating in the work of the therapy group, is one of the most important criterion to consider. A client’s high motivation for group therapy can compensate for other areas of clinical concerns (e.g., shyness, interpersonal difficulties) that might interfere with the group process (Joyce & Marmarosh, 2023). In general, clients who are motivated and believe that the group will be helpful in creating change are more likely to benefit from group therapy (Yalom & Leszcz, 2020).
Interpersonal skills
When assessing a client’s fit for group, therapists should consider their interpersonal competence (Bernard et al., 2008; Joyce et al., 2000), as well as their potential impact on other group members (Rutan et al., 2020; Yalom & Leszcz, 2020). Clients who are seeking therapy to work through difficulties in relationships, who are willing to explore their interpersonal needs, wishes, and fears with others, and who demonstrate self-awareness are likely to be successful in group therapy (Joyce & Marmarosh, 2023). Research on psychodynamic and interactional groups also suggests that a client’s ability and willingness to engage in self-exploration and self-disclosure, and to give and receive feedback has a positive impact on client’s outcome in group therapy (Tasca et al., 2021; Yalom & Leszcz, 2020). Similarly, an individual’s insight into the connections among their interpersonal difficulties, emotions, and symptoms should make them a good fit for group (Crits-Cristoph et al., 2013). Furthermore, certain personality factors, such as extraversion, conscientiousness, and openness may be associated with positive outcomes in group therapy (Ogrodniczuk et al., 2003). Overall, the literature suggests that individuals who are motivated, willing to engage in self-reflection and disclosure, able to tolerate frustration and distress, and have basic interpersonal skills are likely to benefit from group therapy (Joyce & Marmarosh, 2023).
Exclusion Criteria
Exclusion criteria help therapists assess whether an individual might become disruptive to the group process and development of cohesion (Joyce & Marmarosh, 2023). Similarly to inclusion criteria, these criteria are not set rules, but rather guidelines to assist therapists in their selection process. Exclusion criteria often stem from clients’ current clinical presentation. For instance, active substance abuse, acute psychotic symptoms, or the need for crisis-specific interventions would interfere with one’s ability to engage with the group (Joyce & Marmarosh, 2023; Yalom & Leszcz, 2020). Other factors impacting a client’s interpersonal functioning, such as hostility or willingness to engage with the group, should also be taken into consideration. The group psychotherapy literature indicates that low motivation, poor insight, hostility, denial, defensiveness, risky and self-destructive behaviors, and inability to adhere to the group’s norms are typically associated with early dropout from group or poor overall outcome (Brabender & MacNair-Semands, 2022; Joyce & Marmarosh, 2023; MacNair-Semands, 2002; Yalom & Leszcz, 2020; Valbak, 2018).
Therapists should also consider the amount of support an individual might need from the leader(s) to engage in the group. For instance, clients who are interpersonally avoidant or experience intense difficulties engaging with others might not benefit from the group without extensive therapist support. Such clients might need more pre-group preparation to be able to have a more positive experience in group. Furthermore, clients who question the efficacy of group therapy are not likely to benefit from group and will likely negatively impact group cohesion (Joyce & Marmarosh, 2023).
When selecting potential clients for a group, therapists should be aware of the group’s need for a sense of safety. A group member who makes others in the group feel unsafe will negatively impact a group’s ability to become cohesive. For example, Chen and colleagues (2008) noted that groups are social microcosms where external patterns of beliefs, biases, and behaviors are likely to manifest. For this reason, an individual who holds prejudiced beliefs about a marginalized group or lacks cultural humility and sensitivity to the need to empathically explore differences may not be a good fit for a group with diverse members (Joyce & Marmarosh, 2023).
It is important to understand that exclusion criteria might be outweighed by a client’s motivation or ability to engage in the group in meaningful ways (Brabender & MacNair-Semands, 2022). In such cases, pre-group preparation will be key to maximize such clients’ experiences in and contribution to the group (Whittingham, 2018). Finally, when a client is denied participation in a group due to poor fit, therapists should disclose the reasons for the denial in therapeutic ways and recommend alternative treatment options for the client (Joyce & Marmarosh, 2023).
The Selection Process
As noted earlier, the selection process is complex, as many individual and group variables are taken into consideration to determine client-group fit. As a result, Bernard et al. (2008) encouraged therapists to use clinical assessment and empirical measures to assess fit. As a guiding structure, Joyce and Marmarosh (2023) describe two steps to the selection process. The authors recommend identifying exclusion criteria first in order to decide if any factor might disqualify an individual from participating in group. Second, they recommend conducting a more detailed assessment, using empirical measures, to determine whether an individual is a good fit for a particular group and to assess for that individual’s readiness to participate. Brabender and MacNair-Semands (2022) echo this suggestion, positing that using assessment measures in the selection process helps build groups with better attendance and outcomes.
Measures for Client Selection
The following measures are recommended by Joyce and Marmarosh (2023) to assess fit or suitability, and readiness for group:
The Group Therapy Questionnaire-Short Form (GTQ-S; MacNair-Semands, 2019). The GTQ-S is a short version of the Group Therapy Questionnaire (GTQ), which was developed by MacNair and Corazzini (1994). The GTQ-S is a structured assessment of factors typically related to early group dropout. Through open-ended and Likert-scale questions, it assesses variables that tend to impact group behaviors, such as interpersonal difficulties. The GTQ-S is a helpful tool in case formulation, supporting clinicians in understanding group members’ presentation in the context of their personal and family history, interpersonal difficulties, and goals for therapy. By assessing factors often associated with early termination or dropout, the GTQ-S can help group therapists anticipate potential issues faced by clients in the group (Joyce & Marmarosh, 2023).
The GTQ-S includes 25 items organized in five domains: (1) experiences and expectations for counseling (e.g., On a scale from 1 to 7: “I look forward to beginning group therapy”); (2) family relationships and roles (e.g., “What role do you play in your current family or intimate relationships that contributes to problems?”); (3) health and mental health (includes questions about individual health and mental health history); (4) interpersonal difficulties (e.g., “Please check the interpersonal problems you experience.”); and (5) goals, fears, and difficulties in psychotherapy (e.g., “What are your goals for group therapy?”) (MacNair-Semands, 2019). The questionnaire can be completed in about 30 minutes and scored in about 15 minutes. It can be accessed for free on https://www.routledge.com/Core-Principles-of-Group-Psychotherapy-An-Integrated-Theory-Research-and-Practice-Training-Manual/Kaklauskas-Greene/p/book/9780367203092 (under Support Materials tab and in Pre-group 1–10 folder).
The Group Readiness Questionnaire (GRQ; Baker et al., 2013). The GRQ is a brief assessment of client’s appropriateness for group psychotherapy. It was developed from the Group Selection Questionnaire (Burlingame et al., 2011). It evaluates interpersonal characteristics and expectations for group therapy. It can be completed in about five minutes and includes 19 items rated on a Likert scale. The items are divided into three scales: (1) expectancy; (2) participation; and (3) demeanor. The questionnaire is meant to be used as a screening tool to identify clients who might require more pre-group preparation. The measure can be purchased through www.oqmeasures.com.
Therapists should note that measures that are not specific to group psychotherapy can also be used to facilitate the selection process. For instance, assessments of clients’ clinical presentation and symptoms, as well as measures that assess experiences related to identity and discrimination can also be helpful to use to gain better awareness and understanding of what a client might bring with them to group (Joyce & Marmarosh, 2023; Tasca et al., 2021).
Group Composition
The focus of group composition shifts selection decisions from the individual members to the group-as-a-whole. Rutan and colleagues (2020) talked about composition as the “character” of the group. The 2008 AGPA Group Practice Guidelines defined the goal of group composition as “bringing together a mix of individuals who will both challenge and support one another and develop and maintain cohesion” (Bernard et al., 2008; p. 477). In regard to group composition, too much difference between group members can become disruptive to the group, and not enough might not help the group move towards its goals (Rutan et al., 2020). The hope is to find a balance in client characteristics that fosters cohesion and connection on one hand, and encourages members to challenge each other and explore differences on the other.
Although ideal group composition might not be achieved, therapists should be thoughtful in the way they select clients for group. Joyce and Marmarosh (2023) described that process as “actively composing the group” (p.51) to maximize cohesiveness. They note that a well-composed group is more likely to start well and make progress rapidly. To compose a group well, therapists should have a clear idea of what they are intending to create. They should clearly define the type of group they want to run, its goals and work style or process, as well as the framework required. Joyce and Marmarosh (2023) recommend the following guiding question: “What client variable (or combination of variables) is likely to be critical in the group’s development and why?” (p.52). This implies that group therapists should be skilled both in individual case conceptualization and group case conceptualization, as composing a cohesive groups requires to think about individual client presentations, as well as who those will interact in a group (Barlow, 2013).
The aims of the group typically inform composition goals. Therapy groups are often defined as homogenous or heterogenous (Bernard et al., 2008), which can refer to similarities or differences in presenting concerns, symptom severity, psychological resources and ego functions, personality traits and interpersonal styles, as well as demographic and identity variables. In general, groups with more specific aims tend to be more homogenous, particularly with regard to symptom presentation (Joyce & Marmarosh, 2023; Kealy et al., 2016). For example, a group focused on depression will be homogenous in terms of diagnostic and clinical presentation, while a group focused on transgender women survivors of violence will be homogenous in terms of gender identity. On the other hand, process-type therapy groups tend to be more heterogenous with a “balance of characteristics,” (p. 51) such as contrasting attachment styles or interpersonal dynamics (Brabender & MacNair-Semands, 2022; Joyce & Marmarosh, 2023). Therapists should be clear about the goals of their group and the population they intend to serve to compose it thoughtfully. Group composition should be thought through before group facilitators start selecting potential clients.
Composition and Identity
Chen et al. (2008) described therapy groups as a social microcosm. As such, clients often repeat outside behavioral and interpersonal patterns in group sessions (Bernard et al., 2008). This idea applies to dynamics of power and privilege and other cultural issues. Therapists should be especially mindful of these kinds of tensions brought in from the society at large when composing groups. While diversity of identities in therapy group creates opportunities for meaningful exploring of diverse perspectives (Joyce & Marmarosh, 2023), it also increases the risk for dynamics of power and marginalization to be enacted in the group leading to harmful and hurtful conflict or misunderstandings. For instance, groups with diverse members will inevitably involve members who experience racism and members who perpetuate it, as those experiences are “carried into group therapy sessions” (Bemak & Chung, 2019; p. 176). For this reason, it is imperative for therapists to be aware of and understand power dynamics, privilege, marginalization, and oppression and be prepared to explicitly address them. Furthermore, therapists should be aware of their own cultural identities and the impact those have on themselves and their interactions with others and the world around them (Abernethy, 2024; Bemak & Chung, 2019; Joyce & Marmarosh, 2023). They should also be aware of how clients with diverse backgrounds might experience the world. This means that therapists should stay informed about issues affecting marginalized communities and pay attention to how privilege and oppression manifest both intentionally and unintentionally, as well as in obvious and more subtle ways (Abernethy, 2024; Bemak & Chung, 2019). Adopting a multicultural orientation can help therapists provide better group experiences for their clients (Kivlighan & Chapman, 2018; Owen et al., 2011).
Therapists should also note that homogeneous groups composed of members having one saliant cultural identity can be more advantageous in some contexts than groups with diverse client composition (Smith et al., 2011). For example, a university counseling center at a predominantly white institution (PWI) may hold a process group centering the experiences of Black students to create a safe space for them to process their experiences on campus. Such groups can help clients from marginalized communities find support while feeling safe.
Summary
- Therapists can compose groups that are likely to be cohesive and successful by engaging in thoughtful client selection.
- This can be done by being educated about client dynamics that are likely to impact a group’s development, understanding standard inclusion and exclusion criteria, having clear goals and frameworks for their groups, and using clinical judgment.
- This process can be strengthened by utilizing assessment measures such as the Group Therapy Questionnaire (MacNair & Corazzini, 1994; MacNair-Semands, 2019) and the Group Readiness Questionnaire (Baker et al., 2013; Burlingame et al., 2011) to supplement the process, as well as developing skills in case formulation (cf. Tasca et al., 2021).
- Despite careful consideration of client characteristics and the primary qualities of the present or planned group, some mismatches will occur that require thoughtful interventions by the therapist to repair disruption and harm.
Preparation and Pre-Group Training
In the selection process described in the previous chapter, the group therapist decides whether or not to invite a potential group member to join a particular group, a decision based on the therapist’s sense of the goodness of fit between the candidate and a group. However, the decision to accept this invitation is the potential group member’s. This decision needs to be driven by the client’s acquiring a fairly accurate understanding of how the group can be helpful, holding realistic expectations of what can occur in the group (including risks and challenges and how they will be addressed), and developing an appreciation of the work the client will be asked to do in the group. Group therapists also have a responsibility to present this information in ways that are responsive to the prospective members’ presenting concerns, needs, identities, and socio-cultural context.
Pre-group Preparation and Orientation
This orientation phase of group therapy provides a space for the group leader to review the structural parameters of the group—its defined tasks and goals, the patients’ and therapist’s work roles, the frame, and rules—and to speak to the value of adhering to these structures, but with flexibility and attunement to the needs of the group members. Equally important, this is the time to explore and address the newcomer’s expectations and concerns about who the others are in the group and how the newcomer will get along with them. Leaders review what will happen and what kinds of interpersonal tensions are likely to emerge, given the makeup of the newcomer and the ways of the group. There are opportunities here to identify similarities between the newcomer and the other group members, stressing that everyone is asked to work on their psychological problems and to be empathically attuned to each other, thus helping to promote such therapeutic factors as a sense of universality, cohesion, and a shared working alliance. At the same time, preparation needs to entail exploring unique expectations and concerns, including those borne of the individual sociocultural identities of the members. Multicultural (cf. Abernethy, 2024) issues of status, power, privilege, marginalization, and oppression, as they manifest in the group, are integral aspects of the work of the group, so the preparation space can be used to identify the newcomer’s salient identities and begin the conversation of how cultural differences and tensions arising from them in the group can be safely explored and contained.
How to conduct the pre-group orientation should ultimately be guided by the needs of the newcomer and the other group members, needs based on their developmental histories and their sociocultural contexts, as well as the treatment setting (Burlingame et al., 2002; Piper & Perrault, 1989). Clinical judgment should inform what dosage and formats are needed with each client to address any conflicts, anxiety, or misconceptions about what the group experience will be like. Group leaders may choose to conduct multiple preparatory sessions to establish rapport and build an alliance before clients join the group, with recommended structures ranging from a single 30-minute meeting to several sessions, depending on when a client can commit to the rules and roles of the group (Joyce & Marmarosh, 2023; Piper & Perrault, 1989; Yalom & Leszcz, 2020). These preparation sessions can vary in format, from individual one-on-one meetings to small-group orientations that include multiple prospective members, or even an introductory session at the beginning of each group session to help set expectations (Yalom & Leszcz, 2020). Information shared during pre-group orientation can be conveyed through a mix of passive and active methods, including written, verbal, audiovisual, or experiential formats that address behavioral, cognitive, and emotional aspects of psychoeducation (Burlingame et al., 2006; Piper & Perrault, 1989). Active, experiential exercises, such as mirroring a group session through dialectic engagement, behavioral rehearsal, and role-play, can be particularly effective in normalizing the group experience for members (Piper & Perrault, 1989).
The group leader’s own preparation work
While questions of what group therapists bring into the therapy space with them are discussed throughout these guidelines, it is important to note how this applies specifically to the pre-group preparation process. Throughout the assessment and orientation process, therapists should be mindful of potential reactions they might have to prospective clients and where these reactions are coming from. This means that therapists should be doing their own internal work to gain awareness of their own assumptions, expectations, biases, and prejudices.
Further, group facilitators are not immune from the pulls of systemic bias from their own socio-cultural environments. Therefore, it is also necessary for group leaders to engage in self-reflection and personal labor on their own identity development, as well as attend to how identity factors impact group, to minimize harm (Cone-Uemura & Bentley, 2017). There are several questions a group leader can critically reflect upon mindfully:
- What privileged and/or historically marginalized identities do I hold as an individual within our current historical, socio-cultural, and political context? How could this potentially show up in the pre-group meetings, and how can I address this if clinically appropriate?
- How could my identities interact with other intersectional identities (visible and/or invisible) with this particular potential group member or in the eventual group membership?
- What socio-cultural narratives would my actions or inactions potentially reinforce within the pre-group meeting and ultimately the group?
- What assumptions do I hold about what would make a successful group leader, pre-group meeting, and/or group experience? Would these assumptions honor intersubjectivity and members’ adaptations in navigating their socio-cultural systems? How could I assess this in the pre-group meeting?
The tasks of the preparation phase
Forming a working alliance
A primary objective of pre-group preparation is to establish a working alliance between group therapist and incoming client, a shared initial understanding and agreement about the issues to be worked on in the group treatment and a commitment to that work, as well as a mutual trust and emotional bond (Burlingame et al., 2002; Horvath, 2001; Rutan et al., 2020). Creating a strong therapeutic alliance allows for increased positive outcomes in a variety of forms, including increased contribution from group members. It facilitates more open boundaries to take risks and absorb new information in a non-threatening environment.
Specifically, the therapist should clearly convey and explain what the group tasks and process will look like (e.g., exploration of the here-and-now interpersonal dynamics and emerging relationships, sharing of one’s personal needs, feelings, wishes, and fears) and ascertain whether the client is invested in that work (Yalom & Leszcz, 2020). Further, the therapist also needs to help the client understand what the therapist’s work role is. Depending on what schools of psychotherapy and theories that the therapist follows, the therapist’s work role could include reinforcing of therapeutic values and norms, providing a safe and reflective space, offering interpretations of what is happening in the group, or conducting psychoeducation.
The development of a strong working alliance can be supported by therapists demonstrating their investment in understanding the new member’s experience and in formulating therapeutic goals in collaboration. As a starting point, group therapists can gather information about the client’s experience, history, sense of identity, goals for group, and interpersonal patterns of behavior (Rutan et al., 2020). Some literature suggests that utilizing standardized assessments in addition to gathering information through clinical observations and conversations with the client can be helpful in getting better insight into clients’ experiences (Hewitt et al., 2018; Joyce & Marmarosh, 2023; Whittingham, 2018). This information and initial interaction can also be helpful in confirming client-group fit (as discussed in Chapter 1), which is a necessary part of preparation for the group process (Turner, 2017).
Psychoeducation on the rationale for group psychotherapy
One core aspect of the group leader’s role in the pre-group meeting is to offer a rationale as to how group therapy works to alleviate symptoms and create psychological change (Joyce & Marmarosh, 2023; Yalom & Leszcz, 2020), whether it is through acquiring of new experiences of interpersonal relationships, gaining insights into how one is perceived by others, or enhancing one’s coping skills. This work involves helping prospective clients see and understand the relationship between their present symptoms and complaints (e.g., depression, anxiety, loneliness, anger) and interpersonal dynamics (particularly the client’s characteristic wishes, needs, fears, and defenses of self in relation to others). Thus, pre-group preparation can be used to begin to develop a shared formulation on how the candidate’s view of self-in-the-world (i.e., internal self-other schemas or self-object representations or internalized narratives and beliefs about the self) can be expected to get played out in the group and evoke the symptomatic problems that the client is experiencing. During this stage, the therapist can educate the prospective client on how such learning can be used to help the client make changes in interpersonal functioning and views of self-in-the-world.
For example, a new group member’s goal may be to reduce people-pleasing behaviors. The preparation work can illustrate how the group can offer opportunities for the client to experience these interpersonal tendencies or patterns, an understanding of why those practices were developed given their socio-cultural context and early home life, and an invitation to pull against those familiar tendencies in new relationships in the group. That is, the group can be described as a laboratory to explore what it would be like to be less defensive and more authentic in the new interpersonal relationships in the group and discover that the feared and anticipated consequences do not arise. Even if the group member does not progress to the stage of setting boundaries, they may become more aware of when and how they could set boundaries through the interpersonal modeling by others whom they admire within the group. This helps provide multiple scaffolded ways the client can visualize and experience themselves as making progress through the action of group therapy. Each of these reinforce that the goal of the group is to increase flexibility, hope, and possibilities for new interpersonal styles rather than prescribe a correct way to be or show up in the world.
Alternatively, a white transgender male group member who comes from an emotionally abusive family that has consistently misgendered him may enter the group feeling unworthy of love or connection due to critical messages from his past labeling him as “too much.” The group setting can provide a space for him to challenge these internalized narratives about how others perceive his presence. When other group members share how they value his contributions and stories, this creates a counterpoint to the critical voices from his family system. If, however, group members do feel overwhelmed by his interpersonal style and provide him with that feedback, he may gain a more nuanced understanding of what specific aspects of his behavior feel intense for others. The role of the therapist in the pre-group preparation phase is to help the client prepare for this type of feedback by helping them understand that it is an important part of the process. This process could open up new avenues for connection, allowing them to explore alternative ways to interact with others. Additionally, each member may begin to view the group’s reactions as empathically mirroring the trans client’s internal experience, thus providing an opportunity to address these responses with awareness and compassion.
Reducing anxiety about the group
While the idea of group therapy as a healing environment needs to be explicated in the preparation phase, the anxieties, misconceptions, and biases about groups also need to be explored as joining a therapy group can be anxiety inducing for new group members (Rutan & Stone, 2001; Rutan et al., 2020; Yalom & Leszcz, 2020). Being that one of the benefits of a pre-group session is to reduce client anxieties (Burlingame et al., 2006; Rutan et al., 2020), this should be a primary focus for group therapists during this meeting. Specifically, the therapist should address any underlying assumptions about group therapy, such as the belief that group therapy is an inferior form of treatment, concerns that one can lose one’s autonomy and individuality though emotional contagion, fears of rejection or ostracism, or not having enough attention from the therapist (Rutan et al., 2020).
Many group candidates, particularly those from societies that value individualistic as opposed to collectivist values, may approach the idea of group therapy with beliefs that there won’t be enough time with the therapist or that they will have to compete for therapist’s attention. It is crucial to identify this kind of resistance in the preparation work by helping them understand that every moment in the group, if approached with openness and curiosity, can foster growth for themselves and others (Yalom & Leszcz, 2020). The false assumption that the individual member benefits from therapy only when they are the primary focus can lead to the misconception that when attention shifts to others, one’s own growth is stalled. Ormont (as cited in Ferguri, 2001) and others from Indigenous and Afrocentric traditions challenge this view, emphasizing that seeing oneself as separate from others limits the potential for collective healing (Owens et al., 2016).
In reality, one member’s success can inspire sympathetic joy in others, as group members recognize parts of themselves in each other (Ferguri, 2001; Magee, 2019). In pre-group orientation, group therapists must highlight the value of engaging with others in this way, encouraging members to lean in with curiosity about the others in the group and explore the network of relationships within the group and, perhaps, to seek feedback about their engagement in the process of communal sharing. This process helps clients see beyond visible differences, uncovering deeper connections and shared experiences (Hardy & Bobes, 2016; Yalom & Leszcz, 2020).
New group members’ apprehensions about group therapy may be informed by their experience in their own sociocultural context (Holmes, 2002; Leary, 2000; Ogrodniczuk et al., 2004; Rabinowitz, 2001; Wright & Gould, 1996). Thus, considerations of how group member identities and the subsequent interactions of the identities in the room will be processed is important to address in pre-group meetings to reduce such anxieties. Chen and colleagues (2008) encouraged group facilitators to utilize their multicultural competence (MC) with clients in these initial meetings as a method to establish trust, demonstrate their competence, and model how to enter less common conversations that often bring discomfort. In preparing for group therapy, group facilitators should consider each member’s acculturation level, conceptualizations of mental health, beliefs regarding the origins of symptoms, and experience and manifestations of distress in different contexts (e.g., school, family, work). Furthermore, examining the cultural differences in goals, roles, and alliances could be beneficial as this process can reinforce the therapeutic bond (Bernard et al., 2008). Group leaders applying their multicultural competence with group members who are aware of their anxiety (particularly if identity related) can help demystify some of the group experience and give space for identities that may often be ignored outside of the therapy room. When potential group clients are less aware of their anxiety or the impact of their identities in the room, group facilitators can help increase their consciousness of their anxiety to prevent these internal experiences from presenting in therapy in counter-therapeutic ways (Rutan & Stone, 2001).
Discussing harm, repair, and safety plans and tools
Despite the most therapeutic efforts by the therapist and the commitment of the members to work on their therapeutic goals, the complexity of group life will likely lead to instances of misattunement, rupture, and empathetic failure. During the pre-group meetings, group therapists can normalize the possibility that harm can occur. Leary (2000) recommends having candid early conversations, with a frank exchange of views about what people may be concerned about related to group involvement, perceptions of their identities, and otherwise. Such clinical efforts build trust in the therapist as they create an opportunity for the client to feel heard, offer their perspectives, and even provide feedback for the therapist to receive. In these conversations, facilitators can provide examples of ways in which the group structure strives to prevent or reduce the possibility of harm, how issues will be handled if they occur, and what repair can look like in the group. The pre-group meeting is also an opportunity for therapists to hear more about what may help respective clients feel safe in the event of a relationship rupture.
There is a broad base of data reinforcing the critical importance of attending to safety in clinical work. This data includes attention to issues such as microaggressions, microinvalidations, and other types of harm related to identity (Belcher Platt, 2017; Miles et al., 2021; Shelton & Delgado-Romero, 2013; Sue, 2010; Taylor, 2021). It is imperative that group facilitators become familiar with the types of harms that can be experienced by diverse populations and create a pre-group preparation space that is trauma-informed, as described by The National Center for Trauma Informed Care (SAMHSA, 2014). Experiences of microaggressions and macroaggressions (e.g., slur usage or ridicule related to an identity) are a source of traumatic experience for many whose identities have been marginalized (Nadal, 2018). These experiences can have host of negative impacts, including somatic harm (Menakem, 2017; Nadal, 2018). Clinicians can review and incorporate AGPA Guidelines for Creating Affirming and Restorative Group Experiences (2023) to assist in attending to issues of safety inclusive of the potential identities present. These guidelines were developed by AGPA’s Diversity, Equity, and Inclusion Task Force to increase clinician’s awareness of experiences of diverse populations, as well as dynamics of power, privilege, and marginalization. The guidelines provide guidance to clinicians to more effectively address harm related to oppression and marginalization that may arise in group sessions. Informing clients of these guidelines and how they will be incorporated into group practice is an important part of providing an overview, as well as offering reassurance about how the group will attend to safety. In addition, utilization of specific resources that offer tools of prevention, as well as management of harm and safety, are important for clinicians to review and reference (Miles et al., 2021; Nadal, 2018; Sue et al., 2019).
Welcoming the Full Identity
Welcoming the client’s identities and how they impact one’s experience and anticipated interactions in the group is a critical part of the preparation phase. It is important for group facilitators to acknowledge that group members hold a range of identities and that identity is always in play in a group, whether spoken or unspoken, conscious or unconscious, seen or hidden (McGoldrick & Hardy, 2019). The preparation phase may allow a safe and contained initial exploration of whether these identities confer privilege, power, and dominance, or have been marginalized and oppressed, and of the feelings and experiences resulting from such status differentials in society and likely in the group. This means that it is important for therapists to be aware of the interplay between their own held privileged and marginalized identities and those of the clients as they decide what to prioritize with respect to the pre-group preparation. Ribeiro (2021) encourages group leaders to discuss identities and their intersection during pre-group preparation session(s) by:
- Talking with newcomers about the identities they hold;
- Exploring how those identities may interact with others in the group and the group process that results;
- Reassuring clients that all aspects of identity are important parts of interactions in group, including less often disclosed aspects of themselves;
- Reflecting on how identities might impact connection with the therapist;
- Assisting in members’ preparation for self-reflection, as well as connection in the group process.
Reviewing group agreements
The group rules should be reviewed in depth with prospective group members, along with the rationale for these structural parameters and whether the candidate understands them and can abide by them. Typical agreements include:
Accessibility considerations. Whether the group is meeting in-person, virtually or hybrid, making the group accessible to a range of individual needs (e.g., sensory needs, neurodiversity, etc.) is a part of the group leader’s preparation. Accessibility considerations should be clearly communicated to new group members. For example, if running an online group, the clinician can inform prospective members that closed captioning will be enabled, that information typed in the chat (if used) will be read aloud, and that cameras may be turned on or off at times to attend to individual needs. In addition, all material and activities shared during orientation should be accessible to group members with diverse identities and needs (e.g., access to translation, audiovisual resources, etc.).
Informed consent. The therapist needs to help the new patient gain as accurate a picture as possible of how the group will be experienced so that the client can make an informed decision about whether or not to accept the invitation to join a group, as well as to terminate from the group should the group experience not meet expectations or needs (Brabender & MacNair-Semands, 2022 ). The group facilitator(s) should acknowledge each group member’s autonomy to consent to engagement or to set appropriate boundaries within the group process, and reinforce that consent can be adjusted at any time. This assists in reducing the power differentials and acknowledges power dynamics and privilege (Leszcz, 2004).
Confidentiality. The therapist needs to emphasize the importance of privacy, protecting the identities of the group members, and the group’s confidentiality, including what information will be gathered in pre-group work. Participants should be informed about what they are allowed to share, or not to share, relating to group content and how their information and experience will be protected by group members. In other words, what happens in group stays in group. While this is not strictly enforceable except for the therapist’s abiding by confidentiality, the rationale for this rule needs to be stressed, namely its aim is to increase trust in the group process.
Contact outside of group. Therapists need to review how extra-group contact is regarded in this particular group since such interactions are likely to impact the dynamics within the group (Rutan et al., 2020). For some groups, these external interactions may be unavoidable (e.g., colleagues working together, residents or interns in the same or related programs, members of the same church, synagogue, mosque, or ward), or even desirable or encouraged (e.g., BIPOC students at a predominately white institution or academic program where safety, solidarity, and mutual support is of importance), while in other groups they may be discouraged (group focusing on codependency issues). In all situations, clinicians should inform clients about the potential impact of external interactions on group dynamics and the group process and encourage them to bring in material from these external group contacts into the group, lest that material be split off from the inner workings of the group.
Time and space boundaries. It is important for the therapist to let the prospective client know the given temporal-spatial boundaries that define the group but also be sensitive to how comfortably this is experienced. The dominant culture of psychotherapy, often stemming from the ideals of dominant identities in westernized cultures, establishes these boundaries, which may be unfamiliar to and uncomfortable for people from differing sociocultural groups. Historically, therapy has adopted a more rigid view of time, including placing significant focus on start and stop time. Firm methods of attending to time have often disenfranchised and harmed Black, Latinx, Indigenous, Asian, and other People of Color (Liu et al., 2023).
While discussion of start and stop times are a part of creating a stable frame, rigidity on this aspect of group can create excess anxiety, and at times alienation of group members. Reiterating the importance of valuing participant presence and engagement for the time that they are in a group is of importance when discussing time boundaries and can serve as a stabilizing force in the framing process. Providing information regarding the planned start and end time is of importance, as well as discussion of any parameters for flexibility in the time guide. For example, reflect and discuss how group members should alert the group leader if they will be delayed in arrival or if they need to miss a group.
Group leaders should also address how time will be used during group sessions. Factors to consider and potentially address with new clients include:
- Use of the first few minutes of group sessions;
- Making a plan with prospective clients about what to do should they need to take brief breaks (e.g., incorporating pauses for deep breathing and recentering, welcoming stepping away from group for a brief period and returning, etc.);
- Examining accessibility needs (e.g., health concerns and disability needs where individuals may have to stand, stretch, step away from the group for their health and wellbeing in order to participate).
Diversity consciousness and dialogues
Group therapists appear to agree that “a group” represents a microcosm of the larger societal and cultural contexts (Agazarian, 2001; Yalom & Leszcz, 2020). The concept of isomorphy helps group leaders understand that the group, much like the individual member, does not separate themselves from the influence of systemic factors within their sociocultural environment (Riberio, 2021). Indeed, this concept highlights that aspects of oppression (e.g., racism, misogyny, homophobia, transphobia, ableism, xenophobia, etc.) will manifest within the group context, regardless of the precautions and frame taken by the group facilitators in the pre-group meeting. Historically, group therapy has relied on a view of benevolent neutrality, holding that to be objective is to cut one’s bias of thoughts and feelings out of the analysis when engaging in group treatment or intervention, rather than owning one’s subjectivity (Ferguri, 2001; Rutan et al., 2014). This has resulted in a lack of directness with respect to leaning into issues of social justice in group psychotherapy (Dalal, 2002; 2016).
Contemporary practices have been clear in identifying the need to directly address and illuminate the unconscious pulls of systemic issues (Abernathy et al., 2024; Dalal, 2002; Elias, 1994; Kasklauskas & Nettles, 2020; MacNair-Semands, 2007; Riberio, 2021), beginning during the preparation stage. Since there is no escaping the internalized bias, an important goal of pre-group orientation is to bring awareness to the origin of these dynamics and how they can present in group (Agazarian, 2001).
Exploration of privileged identities.
Abernethy (1998; 2024) notes that pre-group preparation can include helping potential members anticipate a group with a range of identities. Safety in the group can be communicated via respect for members’ cultures and identities, both visible and invisible (Stevens & Thijs, 2018). The pre-group meeting may provide opportunities for clinicians to assist clients in understanding the less visible ways that their culture and identities impact how their mental health manifests in their experiences and interactions with others (Miles et al., 2021).
Thus, group facilitators can use the pre-group meeting as a time to prepare group members who seemingly have more historically privileged identities on how they can engage in the therapy space. Specifically, they can introduce that addressing cultural issues will be one of the norms in the group (Bohm, 2010). Facilitators can bring insight that reciprocal conversations about all identities present in the space create group cohesion and greater safety, especially for those who identify as minorities of those respective identities (Chen et al., 2003; Yalom & Leszcz, 2020).
There are several ways that culturally competent group therapists could use the preparation work to support members in understanding where they hold privilege and to provide tools to manage it when it manifests in group therapy sessions. For instance, group leaders could inquire from potential members, “If there was a person in the group who held one type of identity or belief that would make it difficult for you to feel that you could connect to them, what would that identity be?” They could then emphasize the importance of creating space to listen to differing experiences and increase overall openness to other perspectives (Stevens & Thijs, 2018), contingent that doing so would not cause psychological harm to the prospective member. Burnes and Ross (2010) encourage clinicians to make direct inquiries in pre-group meetings about how clients are able to manage conversations around difference and oppression. An example included, “How do you feel when there are conversations about racism or sexism in a group of people?” Burnes and Ross (2010) noted that these efforts to assess how members handle discussions of oppression are foundational to handling issues of social justice in group therapy, which multicultural competent clinicians aim to do.
Being that some group members may have limited insights around the pervasiveness of implicit bias, the group therapist could offer in the pre-group meeting an example of how biases can be unknowingly present in group spaces. Therapists can model in the pre-group meeting how to create space for group members to share their emotions related to experiences of marginalization and discrimination (i.e., anger, anxiety, sadness), as well as emotions or blunting of emotions by group members who have more privileged identities (i.e., shame, confusion).
Exploration of visible and invisible identities
Group leaders can prepare prospective group members to manage conversations that may be activating for them (e.g., sharing of discriminatory experiences) by helping them understand that sharing their reactions can help the conversation to broaden to other relevant experiences in the room (Miles et al., 2021).
Stevens and Thijs (2018) caution against making assumptions around the prominence of certain identities to members. For example, in their writings about a rupture in a racially diverse group, it was noted that the identity related rupture entered the group dialogue because of differences in religion (a typically less visible identity) experienced by a Black female (a generally more visible identity) participant. Thus, it is imperative that group facilitators enter the group with an understanding of the various identities that are of value to their group clients. The pre-group meeting(s) present an important opportunity to inquire about this.
Promoting a sense of universality and facilitating cohesion
All guiding principles discussed throughout this chapter not only prepare individual group members to benefit from the group, but also serve as tools to begin developing a sense of belonging within the group. Joyce and Marmarosh (2023) note that pre-group preparation can set the foundation of a cohesive group by reinforcing the frame and structure of the group (e.g., reviewing group agreements, discussing ways that difficult conversations will be handled by the therapist with the group), and help members feel ready to enter the group space. Further, when preparing to orient new group members, group leaders can be mindful of the importance of helping members understand that they will not be alone in their suffering in the group (Joyce & Marmarosh, 2023; Yalom & Leszsc, 2020) and, therefore, structure the pre-group sessions in a way that will help new group members feel a sense of universality with the group.
Summary
- The main goal of pre-group preparation is to ensure that new group members are ready to engage in the tasks of the group.
- An important focus of the pre-group preparation work is on establishing a positive working alliance between the group facilitator(s), the newcomer, and the group.
- Further, therapists’ responsibility during this stage is to provide group members with all the information that they need to understand the tasks of the group and their role in it.
- Group leaders should review the details of the group agreement to ensure that new members understand the frame of the group and address any anxiety and assumption made about group therapy.
- All of this should be approached with understanding of the impact of power dynamics, privilege and marginalization, and the identities and sociocultural context of each group member.
Group Development
Review of Group Development Theories and Models
Group development refers to the systematic changes that groups undergo in terms of their identifiable and characteristic patterns, themes, and dynamic issues. Understanding group development—where the group was, where the group is presently, and where it is likely to shift to—is important based on the premise that choice of interventions needs to be guided by this awareness of the group’s developmental trajectory. A developmental perspective essentially posits that all groups go through identifiable phases or stages characterized by unique challenges to be faced and mastered, separate from but intricately related to the unique intrapsychic and sociocultural patterns that the members bring with them into the group.
While there is a proliferation of models of developmental change in groups, they tend to cluster around two primary patterns: 1) Pendular or recurring-cycle models that view groups as cyclical, returning to the same themes, patterns, and dynamics throughout the life of the group, working through the psychosocial issues more deeply with each iteration (Greene & Kaklauskas, 2020); and 2) progressive-linear models, which essentially posit that groups universally undergo developmental changes analogous to the human life cycle, having identifiable beginning, middle, and ending phases, each with unique dynamics tensions that need to be resolved (Gibbard et al., 1974a).
One of the best known of the pendular models is Bion’s (1962) work that postulates that groups continuously oscillate between two states of mind, a more rational, work-oriented, and conscious quality aimed at achieving the primary task of the group (the so-called work group) and a less conscious, more emotion- and defense-driven state aimed at warding off existential anxieties in the group (the so-called basic assumption group). Analogous to the interplay of therapeutic work and resistance in individual psychotherapy, the work group and the basic assumption group alternate in prominence and salience at any one moment in the group. A similar conceptualization of group development was offered by Bales (1950), who posited that groups cycle through phases that focus on work that attends to the social-emotional needs of the members.
More prominent in number and newer in construction are linear progressive models, which posit that normal group development occurs in a systematic fashion, moving from one characteristic stage to another (Brabender, 2010; Li, et al., 2021). Each stage is distinguished by particular structures, dynamics, and themes. Arguably, the best known of these is Tuckman’s and Jensen’s (1977) model that posited five stages of group development: 1) forming, where members begin to identify as members of a cohesive group; 2) storming, characterized by tension, hostility, or conflicts among members about what the work of the group is and how to relate to the leader; 3) norming, where members resolve their differences and begin to comply with the group norms and values and work on shared group goals; 4) performing, where members deepen their investment in the task of the group, as well as their relationships with one another; and 5) adjourning, where members confront feelings of separation and loss, as well as consider how to use what they have learned in the group going forward (Brabender, 2010; Li, et al., 2021).
Several variations on this original model have been introduced into the literature, namely:
- A four-stage model (MacKenzie & Livesley, 1983, MacKenzie, 1997), positing an initial stage of engagement, where each member works to achieve a sense of belonging within the group; followed by differentiation, where members acknowledge their differences, leading to tension and hostility; then a stage of interpersonal work, where group members explore highly personal experiences and engage in the work of the group; and a final termination stage, similar to Tuckman and Jensen’s (1977) model.
- Wheelan (2005) proposed an integrative model of group development comprised of five developmental stages of dependency and inclusion, where group members rely on the group leader to know what to do in the group and how to feel safe and included; a counterdependency and fight stage, where disagreement emerges within the group regarding shared goals and group structure; followed by trust and structure, where cooperation between group members increases; then work and productivity, where the focus shifts towards the group goals; and finally termination, where the group explores separation.
- More recently, Brabender and Fallon (2009) also proposed a five-stage integrative model, consisting of stages of formation and engagement, conflict and rebellion, intimacy and unity, integration and work, and termination. This model specifies a range of interventions within each stage to enable members to complete the tasks and resolve the conflicts of that stage (Brabender & Fallon, 2009).
Clearly, progressive stage models dominate the clinical-theoretical literature; unfortunately, at this point in time, there is little guidance as to which of these conceptually similar models is best suited for any particular group. Brabender and Fallon (2009) have identified several common conceptual features of progressive stage models. First, in normal development, groups are thought to proceed through an invariable sequence of stages. Thus, earlier psychological tasks, issues, and tensions that characterize any one stage of development must be resolved, worked through, or contained in order for the subsequent stage to emerge. Second, there are a variety of thematic features that distinguish each stage from the other stages. Each stage also has a set of norms or implicit rules about what behaviors are or are not acceptable, and at each stage, the group has a set of competencies that make it possible to perform certain tasks and not others. Third, groups proceed through stages at different rates, sometimes becoming fixated at a certain stage or regressing to an earlier stage. Finally, as groups proceed through the developmental stages, they become better able to accomplish the tasks and fulfill the goals established for the group.
Understanding and Facilitating Group Development from the Multicultural Dimension
The literature on group development has only recently begun to explore the role of multicultural factors in group development and specific practice recommendations for group practitioners from this perspective. In this section, we employ the progressive four-stage model (MacKenzie & Livesley, 1983) to discuss how multicultural factors may be manifested in each stage, and then we present some culturally minded practice recommendations for clinicians to better assist the group in completing the developmental tasks in each stage.
Stage 1: Engagement
MacKenzie (1997) describes this stage as the work of fostering a sense of cohesion and developing alliances to the goals of the group and to its therapeutic relationships. By the therapist’s reinforcement of such therapeutic norms and values as authentic self-disclosure, empathic attunement, and acceptance, members can begin to feel that the group is a safe, welcoming space and thus can enhance their commitment to the group and its work.
Multicultural Characteristics. In the beginnings, much is unknown—what to say, how to relate, how not to get hurt—and members are likely to experience several sources of anxiety. There is also uncertainty about the group’s explicit or unspoken rules for engaging in culture/identity related conversations. Group members may likely navigate the early sessions by staying on the surface level or playing on the safe side, interacting in socially acceptable or accustomed manners and avoiding deep personal expressions or disclosures. For individuals with privileged identities, this may be manifested in their conformity to political correctness, whereas individuals with marginalized identities may show caution or constraint in self-disclosure or emotional vulnerability. The culturally competent therapist needs to appreciate that identity-related power dynamics (i.e., power/privilege and marginalization/oppression) can become enacted from the very beginning of the group and constantly negotiated throughout the group development process. Observations about which members often initiate or direct the conversation, which members tend to take up more space, and which members seem to command more group attention can proffer important insights about the power structure being formed in the group given everyone’s unique composition of privileged and marginalized identities. In the early life of the group, the members may rely heavily on the leader (Yalom & Leszcz, 2020) for the establishment of explicit or implicit group norms around cultural identity conversations. For example, if the leader quickly directs the group away from a potential identity-related conversation in this engagement stage, the group members may learn (often subconsciously) that such topics are not to be broached in this group. Or, if the leader fails to support group members with marginalized identities during a conversation relevant to their identity, those members may feel that the group has an unsafe atmosphere and withdraw from such conversations in future sessions.
Practice Recommendations. Consistent with other theoretical writings (e.g., Yalom & Leszcz, 2020), the primary task for the engagement stage is for the clinician to assist the group in developing a supportive, nonjudgmental, and respectful climate, balancing the work of psychological and sociocultural exploration with the needs to maintain the safety of and to foster the cohesion of the group. Given the group’s reliance on the leader for structure and direction at this early stage of the group (Yalom & Leszcz, 2020), it may be helpful for the leader to explicitly invite members to discuss what group safety and cohesion mean for them individually, including with regard to their cultural identities.
Second, in this initial phase, the clinician could usefully facilitate the establishment of group expectations, norms, and rules conducive to the constructive exploration of multicultural issues (Kivlighan & Chapman, 2018). This may include recognizing that all members of the group possess unique identities that need to be respected and valued, modeling and encouraging an open, curious, and nonjudgmental attitude towards others’ as well as one’s own individual subjective reactions and experiences based on unique constellations of intersecting identities, actively exploring multicultural and identity-related topics in the group instead of ignoring or shunning them and a group commitment to be supportive of members with all types of marginalized identities. The last point is especially important, given the historical and systemic discrimination and oppression experienced by individuals holding any type of disadvantaged identities. This entails ensuring the group’s awareness and acknowledgment of such historical and identity-based trauma (e.g., racial trauma), explicitly expressing a commitment to support individuals holding such identities, and holding groups with dominant identities to account for oppressive acts. These group norms and commitments may be instrumental in avoiding further harm to culturally marginalized group members.
Third, as emphasized by other theorists (e.g., Yalom & Leszcz, 2020), psychoeducation may be helpful in orienting the group members towards the goals and processes of group therapy, including the exploration of cultural identities and differences. For instance, the clinician may discuss with group members the likely reenactment of cultural dynamics within the group that mirrors their outside-of-group dynamics in other social contexts. Then, the group facilitator can further direct the group to discuss necessary safety guardrails in approaching multicultural and identity-related topics within the group so that constructive, albeit possibly uncomfortable, conversations about cultural identities can occur. It is important to note that safety is experienced differently, or may even be in conflict, depending on our privileged versus marginalized identities. For example, for someone with a privileged identity, safety may mean expression of one’s true thoughts and feelings without the fear of being judged or shamed. However, for an individual with marginalized identity, safety may mean not having to be always vigilant in the group about insensitive or discriminating comments that can trigger their historical, identity-based trauma (e.g., racial trauma). These different or even conflicting experiences and needs for safety in the group may require the clinician’s heightened awareness; and explicit explorations about how to approach these cultural issues in the group can be beneficial for the initial engagement stage.
Stage 2: Differentiation
The differentiation stage is marked by the emergence of interpersonal conflict in the group and increased focus on differences between group members, including differential relations to the authority of the group therapist. This stage is worked through when the group is able to develop new ways to tolerate the tensions and work through conflicts (MacKenzie, 1997).
Multicultural Characteristics. As pointed out by group theorists (Brabender, 2010; Yalom & Leszcz, 2020), this stage is characterized by themes of differentiation or conflict among group members or between members and group leader(s). From a multicultural perspective, group members may become more outspoken about their own experiences, perceptions, and beliefs related to culture- or identity-related topics. Alternatively, group members may also become more reticent about multicultural issues if they do not perceive the group to be sufficiently safe and supportive. In any case, with or without the explicit expression of differing views and experiences in the group, members may feel an elevated emotional arousal during this stage. Especially worth noting is that from a trauma-informed perspective, marginalized group members may re-experience their identity-related trauma (e.g., racial trauma) (Comas-Díaz, et al., 2019) in the group when microaggression, invalidation, or even explicit discrimination that one often encounters in daily life is reenacted in the social microcosm of a therapy group (Yalom & Leszcz, 2020). Unsurprisingly, possible interpersonal conflicts and ruptures around cultural identities may ensue.
Practice Recommendations. Given the potential tension, conflict, and rupture in this stage, a crucial task for the group is to navigate the potential cultural impasses, microaggressions, and ruptures (Kivlighan & Chapman, 2018). For clinicians, acknowledging and addressing the differences in group members’ cultural identities or any conflicts or ruptures that arise may be especially important at this time. Ignoring or dismissing the relevance of multicultural identities is a repetition of ineffective avoidance that often happens in daily social contexts and is a loss of therapeutic opportunity to facilitate corrective experiences in the therapy group.
Confronting and addressing these types of cultural identity-related tensions and conflicts within the group can be challenging and anxiety provoking for any group practitioner. While it certainly requires skills and experiences in group therapy, we believe that the process may come down to the basic aspect of holding both while addressing cultural tensions, conflicts, and ruptures. This means that the practitioner may strive to facilitate a group climate that supports and empowers group members with marginalized identities, without shaming the ones with privileged identities. For the first part, it may be beneficial to adopt a trauma-informed perspective with heightened awareness of the historical and socio-political trauma that people with marginalized identities are exposed to in daily life (e.g., colonial occupation of Native American land, historical enslavement of the African American population, legal/societal assault on rights of LGBTQ and gender non-conforming individuals, Anti-Asian violence and racism during the COVID pandemic, antisemitism). Such a perspective and awareness can help reduce harmful labeling or judgments, such as “you are being oversensitive” or “you overreacted” in the group. It may also be important to hold members with privileged identities to task in identifying when and how such microaggression or invalidation come up in the group and take personal responsibility in preventing them.
The clinician may also consider several strategies to curtail shaming that often stalls the learning and empathy development in people with privileged identities. One strategy is to differentiate intention from impact (Sue et al., 2019) so that group members learn to gradually comprehend that what one intends may often differ from how one comes across, and both perspectives can be valid at the same time. It may be also beneficial to discuss how individuals are impacted and shaped by the cultural socialization processes (e.g., racial socialization processes). Recognizing that we all grow up within this larger cultural backdrop and are shaped by the influential external forces of socialization, the group may assist members with privileged identities to acknowledge the societal influences and also accept personal responsibilities when confronted with their own biases, rather than having the knee-jerk “I am bad” reaction and the concomitant defensive attitudes. From an intersectionality perspective, an individual may be privileged in some identity aspects but marginalized in others. The group leader may invite members to reflect the different experiences at different positions of their various identities and use shared experiences to facilitate understanding and empathy. Maintaining a cohesive and containing atmosphere within the group is critical to the holding both work during this stage, often characterized by polarizing us versus them processes, and to the perceived safety of the group.
Stage 3: Interpersonal Work
In this stage, the focus shifts to the deepening exploration of the members’ maladaptive interpersonal patterns (Tasca, et al., 2021) entailing their idiosyncratic wishes, anxieties, and defensive needs as they get deployed and enacted in the here-and-now of the group. Members can check their long-held assumptions about interpersonal relations with how others in the group actually perceive and experience them, thus potentiating opportunities for new interpersonal learning (MacKenzie, 1997).
Multicultural Characteristics. Progressing from the differentiation stage to interpersonal work, group members explore highly personal experiences “in a more vigorous manner” (MacKenzie, 1997; p. 279). Specifically, the task of the group shifts from simple self-disclosure and identifying new ways to resolve conflicts to deep exploration of individual presenting concerns and increased authentic and empathic connection among group members. Regarding cultural identities, members may start to address, rather than just express, their differences in cultural experiences and perspectives with an attempt to work through the group tension and conflicts in a constructive way. This stage may also witness a shift from a group focus to an individual focus (Brabender, 2010), where members try to explore and understand the underlying reasons for one’s unique cultural experiences, given their intersectional identities, which may have contributed to their individual perceptions and reactions in the group around identity-related issues. With sufficient openness, cohesion, and commitment, group members may develop deeper insights both intrapsychically about their own psychodynamics and interpersonally about the way they relate to and differ from each other given their identity similarities or differences. As mutual understanding increases, conflicts may be worked through, and group members can potentially obtain deeper cultural awareness and establish greater perspective taking and emotional empathy. During this process, the group may also reaffirm its commitment to be a culturally safe and brave space, where challenging conversations and corrective experiences around cultural identities can happen.
Practice Recommendations. As group members work through the cultural differences and even tension/conflicts and move to deeper interpersonal work, the clinician may make use of this therapeutic opportunity to facilitate positive changes intrapsychically and interpersonally. Intrapsychically, the clinician may find it beneficial to help members realize the broader cultural and socio-political backdrop that has been shaping every individual’s perceptions, reactions, and responses, thus raising awareness about social-political-cultural influences, as well as personal choices and responsibilities (e.g., understanding an African American group member’s habitual feelings of anger and distrust in the group with the awareness of the anti-Black racism prevalent in the member’s daily life). This cultural lens expands the focus on early environment or interaction with primary caregivers, traditionally emphasized in psychodynamic-interpersonal approaches to psychotherapy (Summers & Barber, 2010; Tasca et al., 2021a), and incorporates the cultural and systemic factors into the understanding of one’s development of internal working models and relational patterns.
Interpersonally, the clinician may identify interpersonal processes within the group social microcosm to facilitate cultural corrective emotional experiences. For members with marginalized identities, such corrective cultural experiences may be the attainment and expression of in-depth understanding and empathy about their lived experiences, and respect and appreciation of their marginalized cultural identities in the group. Additionally, another corrective cultural experience may be the genuine, non-performative acknowledgment and apologies for cultural microaggressions/invalidations and an explicit effort to take personal responsibilities in making future changes from members with privileged identities. For people with privileged identities, the corrective cultural experiences may be the increased awareness and understanding about others’ lived experiences they were previously oblivious to because of the protection of privilege and deeper empathy and connection on the personal, humanistic level. Such learning may happen in a group climate that challenges people with privileged identities out of their zone of comfort, denial, or oblivion without the counterproductive shaming or guilt-tripping.
Stage 4: Termination
The focus of the termination stage is on the ending of the group and how to manage themes associated with it (e.g., ending relationships outside of group, experiences of separation and loss, saying goodbye, reviewing what has been learned, and what work remains) (MacKenzie, 1997).
Multicultural Characteristics. As in the typical ending sessions of any psychotherapy group, in the termination stage group members grapple with a range of cognitive and emotional reactions evoked by separation and loss (Brabender, 2010). The group may also show certain dynamic patterns characteristic of earlier group stages (e.g., withdrawal in the engagement stage, or conflict in the differentiation stage). Cultural identity-related themes may not necessarily be the focus of the group during this stage; however, it is likely that these topics re-emerge when members look back and review their journey in the group where cultural identity has taken the spotlight in previous sessions.
Practice Recommendations. At this ending stage of the group, it is important for clinicians to pay attention to re-emerging culturally specific themes around termination. For example, group members may have reactions (e.g., sadness, fear, etc.) about leaving the group, in which they have had a higher level of safety regarding their marginalized identities but needing to now face the realities in the external world, where discrimination, oppression, and identity-based trauma could be experienced without the therapeutic environment to work them through. Thus, group clinicians may focus on translating the in-group cultural learning experiences into outside-group future plans. The clinician may invite group members to reflect and discuss how each group member can use their learning in the group to facilitate meaningful changes in their life, such as externalization of internalized oppression and self-empowerment for individuals with marginalized identities and engaging in ally-ship work and building more culturally constructive environments outside of group for individuals with privileged identities.
Summary
- Group development models provide important information to help group leaders conceptualize the trajectory of their therapy groups.
- By adopting a developmental perspective, group leaders can gain better understanding of what is occurring within a therapy group and implement interventions that target the specific developmental stage a group is in.
- There are two basic models of group development, the cyclical perspective and the linear progressive. Group therapists should familiarize themselves with these conceptualizations to better respond to the needs of the groups they lead.
- There is limited literature on the application of group developmental models to address multicultural issues common in group therapy. This chapter provides important information to contextualize these models in the sociocultural contexts of group members.
Group Process
The definition of group process depends on the clinical context and the theoretical orientations of those who are referring to it. In general terms, process can be distinguished from content, the latter referring to what is said or done (i.e., the overt verbal and nonverbal behaviors in the group), while the former refers to the inferred emotional needs, desires, fears, and defenses that motivate these behaviors and that get deployed or enacted in the social field. The exploration of group process is important in all therapy groups to optimize task achievement and ensure members’ sense of safety and well-being. This chapter first reviews the three classical and historic ways that process has been conceptualized and then discusses more recent contributions about the role of sociocultural influences on group process.
Work-oriented processes
The therapist needs to keep in mind what the main purpose or primary task of the group is (e.g., psychoeducation, symptom alleviation, behavioral change, or acquisition of new insights) and have a coherent theory about what needs to be done to promote its achievement. Clarity about what constitutes therapeutic work for each individual group participant, for the group-as-a-whole and for the group therapist is important to help the group stay on task. The ongoing monitoring of work-oriented processes (such as the teaching and learning about coping mechanisms in psychoeducation groups or the acquisition of insights into conflictual interpersonal patterns in psychodynamic groups) helps to ensure that there is sufficient conscious commitment, collaboration, and cooperation with respect to the primary task and work of the group, however they are explicitly defined.
Analogous to the notion of therapeutic alliance in individual psychotherapy, in the group setting, the leader needs to consider such questions as, “How are all of us feeling about the group?” and “How invested are the members in the work of the group?” to assess the overall positive identifying of the members with the group and the level of their engagement to its work. Operationally, work-oriented processes have been assessed by such measures as the Engagement scale of the Group Climate Questionnaire (MacKenzie, 1983) and the Positive Working scale of the Group Questionnaire (cf. Miles, et al., 2023). More generally, it is useful to monitor the overall quality of the relationships in the group, as defined by measures of cohesion and therapeutic alliance, given that these measures are strongly correlated with task achievement (Burlingame & Strauss, 2021). The leader can attempt to foster productive and work-oriented interactions among group members through modeling, praise, and the positive reinforcement of therapeutic norms (Bieling et al., 2022) or, alternatively, by the exploration and interpretation of those antitherapeutic processes described below that interfere with task accomplishment. The aim here is not to completely rid the group of these non-work processes but rather harness them in the service of work. While the group’s capacity to engage in the work directly impacts therapeutic outcome (Beck & Lewis, 2000), the therapist should strive for therapeutic progress at a pace that participants can withstand and embrace.
Transference Dynamics
In groups that are characterized as psychodynamically oriented, process-focused, exploratory, or unstructured, the core therapeutic work is the identification of individual member’s underlying early needs, affects, anxieties, and motivations as they are manifested or inferred in the interpersonal relationships in the group. More specifically, this work is thought of as a two-tier process of observing the emergent interpersonal patterns followed by the inferring of what these arrangements signify in terms of underlying needs, wishes and fears (cf. Tasca et al., 2021a). That is, the therapeutic aim is to link the here-and-now group relational patterns with the internal early past worlds of the individual group members.
From this theoretical perspective, central questions for the therapist to contemplate are: “What are each member’s perceptions of and emotional needs and reactions vis-a-vis others in the group?” “What kinds of anxieties are the members experiencing and how are they coping with them?” and “What do the members need from me at this moment to feel less anxious?” To paraphrase Bion (1961), the therapist needs to explore what roles members are implicitly being invited to play to gratify specific emotional needs and contain anxiety. The key conceptual tool for this kind of deep exploratory work is that of projective identification (Horwitz, 1983; Shay, 2011; Weber, 2014). To render the group more familiar and less threatening, members are thought to transpose their internal worlds of schemas and scripts onto others in the group and develop relationships on the basis of those endowments. Analysis of these transference dynamics (i.e., reliving and re-experiencing past relationships in the present) can serve therapeutically by freeing patients from unwittingly repeating the same interpersonal patterns, scripts, and schemas learned early in life and enabling them to develop more adaptive, accurately understood and consciously determined relationships in the present. Identifying the covert, early internal relational patterns that have been projected onto the group helps patients understand why these interpersonal styles originally developed, what purpose they served in the past, especially in terms of self-protective and self-preservative needs, and whether they are still useful in the present, thus providing opportunities for personal growth and new narratives.
Regressive Group-level Processes
Beyond the enactment of individual transference dynamics, all groups, especially relatively unstructured groups, can reactivate developmentally primitive self-other templates and early defenses based on splitting that can be projected onto the group, in concert with other members in the group (Kernberg, 1980). These socially shared and collusive processes serve to contain the inherent existential anxieties attending group participation by rendering the group into more easily comprehensible and familiar, less threatening, and more gratifying social field. Members need not painstakingly work at empathically connecting to separate autonomous others on a rational task but can reduce the inherent complexity of group life by collectively creating a simplified world of good and bad, idealized and devalued, powerful and diminished member roles or subgroups. While serving to allay anxieties, it is important for the therapist to keep in mind that these processes can thwart, sabotage, or divert the rational purposes for which the group is convened. Their identification and containment, what Bion (1961) called “harnessing,” are critical functions of the group therapist who needs to distinguish them from work-oriented group processes.
The clinical literature has described the many ways that these regressive forces shape the experience and construal of the group-as-a-whole and the quality of the members’ relationships to each other (Greene, 1999; Greene & Kaklauskas, 2020):
Group-as-a-whole processes
Bion’s (1961; Rioch, 1970) three basic assumptions constituted one of the first conceptualizations of regressive processes in groups. In essence, these are shared emergent fantasies about the real purpose of the group, namely relating as if the primary goal is to be taken care of by an omnipotent leader (dependency basic assumption), or relating as if the paramount need is to identify an enemy to fight off or flee from (fight flight basic assumption), or relating under the collective belief that an identified couple in the group will magically and miraculously save the group (pairing basic assumption).
Me versus we
A universal dilemma and dialectic in all groups is said to exist between the wish to preserve a sense of self as individuated and apart from the group entity, on one hand, and the need to be an integral and fully connected part of the group, on the other (Greene, 1983). Group processes can be viewed as an ongoing oscillation between these two desires of the human condition. However, if too great, the experience of separateness and distance from the group can evoke anxieties over abandonment and rupture of connection. In turn, these anxieties can trigger restorative fantasies of merger and fusion, which if too great or prolonged can lead to anxieties over loss of self-definition and autonomy. A number of conceptual terms have been developed to capture the experience of fusion and dissolution of self-boundaries, such as Hopper’s (2003) massification, Turquet’s (1974) basic assumption oneness, Hartman’s and Gibbard’s (1974b) group as utopia, and Janis’ (1972) groupthink. On the other end of the continuum are terms that capture the experience of estrangement and disconnection from others in the group, such as aggregation (Hopper, 2003), fragmentation (Springmann, 1976), disarroy (Turquet, 1974), and basic assumption me-ness (Lawrence et al., 1996). The challenge for the group therapist is the ongoing need to monitor and regulate the group members’ experience of cohesion, which is important for task achievement without leading to either extreme of loss of self-boundaries or loss of self-other connection (Burlingame et al., 2019).
Good group-bad group
The member’s relationship to the group-as-a-whole can range from experiencing the group as “the good mother,” nurturing, protective and needs-satisfying (Scheidlinger, 1974), to the anti-group (Nitsun, 1996), destructive and dangerous. It is clinically useful for the therapist to monitor how the group entity is experienced by the members (cf. Greene, 1999). Do they positively identify as being a member of a valuable group that can offer a sense of well-being, purpose and connection? Do they feel safe, protected, nurtured, comforted, uplifted?
Dysfunctional subgrouping
To cope with group-induced anxieties, groups might collusively form us-versus-them polarities and splits within the group. Disowned aspects of self, in concert with other participants, are externalized into some other segment of the group, resulting in what is referred to as dysfunctional subgrouping (Agazarian, 1997). At times, these clashing subgroups can take on a sociopolitical cast, as in the conservatives versus the liberals subgroups. It is important for the group therapist to monitor potential polarizations and how their manifestations can be harmful to individual members, to the sense of group cohesion and to task accomplishment.
Irrational role formation
The emergence of the scapegoat (Horwitz, 1983; Moreno, 2007) and other nonrational restrictive, delineated member roles, such as the spokesperson, hero, provocateur, and difficult patient (Bogdanoff & Elbaum, 1978; Rutan, 2005), are prominent group phenomena. It is important for the therapist to understand that these roles develop as a result of collusive enactments, co-constructions, or mutual projective identifications between the individual and the rest of the group (Gibbard et al., 1974b). That is, the group member taking on one of these roles can be regarded as a ‘container’ for disowned and projected parts of the inner life of the other members and thus speaks on their behalf. Thus, these roles, while often experienced by others in the group as disruptive, may serve important functions for the entire group, including speaking the unspeakable, stirring emotions and revitalizing the group, carrying unacceptable and disavowed aspects of others, and even creating a sense of hope (Shields, 2000).
The therapist’s rational work role also may become endowed, via members’ projections, with either all-good, idealized, or all-bad, persecutory attributes, potentially resulting in non-therapeutic and collusive countertransference enactments vis-à-vis the group membership. The management of the therapist’s countertransference, through the processes of containment, metabolizing, and making meaning of the group’s projections, is related to positive therapeutic outcome (Gelso & Kline, 2022). Management, as opposed to acting out, of countertransference in the group setting is more difficult than in individual therapy, however, because of the multiple and shared transferences directed towards the therapist. It is paramount for the leader to distinguish whether the emotional reactions to the members emerge from the therapist’s internal world and personal history (subjective countertransference) or are induced from the projective processes directed towards the therapist (objective countertransference) (Counselman, 2005). The capacities to reflect on one’s own inner world, to be deeply self-aware, and to control reactivity, defensiveness, and emotional discharge are essential to this work, lest the therapist lose the capacity to remain the rational work leader of the group.
Culture meets the clinic: The growing awareness of sociocultural processes in group therapy
Traditional Western forms of psychotherapy, including group psychotherapy, have largely “decontextulized, ahistoricized, and depoliticized” formulations about psychological development, analyzing patients’ narratives solely from the perspective of the individual within the immediate family of origin without taking into account the sociocultural and sociopolitical contexts, including issues of societal power and privilege, in which they were formed (Tummala-Narra, 2021. The literature now reveals a growing awareness of the role of cultural influences, experienced directly by the individual via such societal channels as church, school, community, and the media and also as transmitted intergenerationally through the individual’s family. There is a burgeoning appreciation of how the socialization experiences and identifications with one of more cultural groupings create the narratives that shape beliefs, values, customs, and life choices and significantly impact the individual’s relationships, including relationships to self, to the therapy group, to other group members and to the group therapist. What happens in the therapy group needs to be considered not only from the perspective of the developmental trajectories and psychological histories of the participants but also from the perspective of the group members’ salient identifications with multifarious sociocultural groupings, each with their imperatives, injunctions, proscriptions, and prescriptions about how to be, what to do, and what to believe. Skilled group leaders must become knowledgeable about how historical and current traumatic experiences and everyday exposure to aggressions and other forms of oppression based on one’s cultural affiliations can contribute to psychopathology.
The literature provides useful illustrations of how prototypical group processes, such as the emergence of a problematic member like the monopolizer, provocateur, or scapegoat, can be understood not only as driven by the enactment of early life scripts acquired from experiences within the family of origin but also from the vantage point of cultural identifications and manifestations of tensions and dynamics within the embedding society (cf. Rigg et al., 2020).
The cultural identities enacted in the therapy group, whether they be based on race (Bemak & Chung, 2019; Hopson, 2024), nationality (Fei et al., 2023), socioeconomic status (Aron & Lefay, 2024), religion (Cornish et al., 2014), gender (Farhoudi et al., 2023), or many other categories (cf. American Psychological Association, 2017) and their combinations and intersections pose two primary challenges for the group therapist. First, the therapist needs to be aware of and curious about these culturally based identities, entailing an appreciation of how culture shapes values, beliefs, and worldviews, including attitudes and affects about psychotherapy and goals of treatment. Second, the therapist needs to contain cultural differences in the group and the ensuing dynamics pertaining to these differences, including issues of power, privilege, oppression, traumatization, and othering operating in the larger society lest they lead to ruptures that negatively impact well-being, fractioning of the group, and interference with task achievement
Knowing the other but not othering
Regarding the first of these challenges is the paramount need for therapists to attend to the cultural identifications of their patients, as well as their own cultural lenses. As Fei et al. (2023) put it: Therapists need to explore differences in the subjective experience of relationships, “what we anticipate from one another in ongoing interaction, how we are socialized to respond to others, and the categories that exist for how we understand who others are in relation to us. Perception, feelings, and responsiveness are highly individual and are also shaped by cultural dictates that organize personal experience (p.7).” “Individual subjectivity is embedded in and not detachable from cultural and historical contexts (p.25),” in essence a view that asserts that the psyche and the social are integrally related. “To narrate the other, we are confronted with the challenge of holding in mind two contrasting narratives, one that translates the other into our own terms to make the incomprehensible coherent, and another that tries to imagine the narrative from the other’s point of view (p.8).” It is important to understand that the therapist need not have complete mastery about the culture of the other but to remain open to learning about the other’s cultural perspective. The therapeutic work is empathic engagement, and at the same time, the therapist needs to remain alert to those processes that interfere with empathy, including reliance on taken-for-granted assumptions, use of stereotypes, complicit othering from a position of superiority or power, or being too quick at pathologizing.
Multicultural orientation (MCO) in group therapy
A multicultural orientation has been developed, both conceptually and empirically, as a core aspect of therapeutic work. MCO as recently applied to the therapy group (Kivlighan & Chapman, 2018; Kivlighan et al., 2019) refers to both the therapist’s and the group’s attunement to relevant cultural issues and dynamics in session. More specifically, it entails three conceptual-clinical dimensions to assess this attunement: cultural humility, referring to the therapists’ and group’s levels of openness, nonjudgmental attitude, and authentic curiosity regarding members’ cultural backgrounds; cultural opportunities, referring to the levels of engagement of the group and the therapist with culturally relevant topics emerging in the group; and cultural comfort, referring to the degrees of nondefensiveness of the therapist and group in attending to culturally charged disclosures.
The very first step toward cultural competence for the therapist is to engage in ongoing explorations of one’s own cultural identifications and how they might impact views of self, others, and the world (Miserocchi & Leit, 2024; Mosher et al., 2017). The therapist might ask “How do my own identifications shape my worldview and create blind spots that might impede the therapeutic alliances and interfere with accurate empathy?” MCO in the therapy group offers a helpful and remedial approach to avoid the harm of othering because it involves both critical self-reflection and openness and curiosity to learning from others.
It is important to note that one will never be fully multiculturally competent, as learning about oneself, one’s culture, and the cultures of others is a lifelong process. Moreover, the kind of change in developing greater awareness and letting go of one’s own idiosyncratic ways of seeing self and other and being open to seeing new world orders is neither easy nor comfortable to achieve for it can arouse existential dread at the thought of being replaced, of losing the familiar and known social order and accepting the chaos of tolerating cultural differences (Hopson, 2024). It is useful to be reminded, as Hopson does, of the therapist’s holding faith for the group, that a way of being and a way of being together, which does not dehumanize, demean, and divide, is possible, that all members of the group can be encouraged to live their true selves, and that relationships can be genuinely and authentically developed on the basis of appreciating both difference and commonality.
Differences contained, not denied
Challenging work for the therapist is to contain the cultural differences in the group lest they become cultural divides, faultlines (Kivlighan et al., 2024), or ruptures (Miles et al., 2021). These destructive group processes can and do readily occur because of power dynamics, othering, marginalization, re-traumatization (cf. Kinouani, 2020; Stevenson, 2022), and the emergence of intense affects, such as rage and shame given the differential value and status that society places on those cultural differences (cf. Hays, 2016). Layton (2021) suggests that differences serve as the boundary across which splitting and projection occur; undesirable, disowned, negative traits or qualities are placed into the Other, forming social hierarchies of superior/inferior, privileged/oppressed, dominant/marginalized. Assumptions about people from diverse cultures, implicit biases and judgments about superiority and inferiority, and stereotypic perceptions of cultural differences can all operate outside of awareness of all or some of the group participants. Kauklaskas and Nettles (2020) say “Prejudicial ideas about others and ourselves form early in life and become procedural and unconscious (p. 34).” Enactments of these attitudes and perceptions in the group are the basis of microaggressions and dysfunctional subgroup clashes, destructive processes which damage the well-being of the participants and the group-as-a-whole and need to be competently managed.
The therapist’s task is to balance the holding, containing, and encouraging of exploration of differences, even as tension increases, with tension regulation, helping the patient and group titrate such feelings as shame and rage. If tension is too high, the mind stops thinking and exploring, and the brain and body go into fight-flight mode. The therapist needs to actively identify and not avoid or deny the cultural undercurrents and perturbations in the group by suggesting that their exploration can be productive, encouraging the group to continue moving, assuring that the therapist is watchful to prevent injury to group members, and offering faith and hope that the changes in the group and group members will be positive. The work of the therapist is to maintain confidence in the ability of the group to work through what is necessary for the group members to achieve fuller authentic personhood, and for the group-as-a-whole to be a place of inclusion and belonging (Hopson, 2024).
Fortunately, the clinical literature, both general and specifically group therapy, is increasingly providing conceptual frameworks and technical strategies to help with the difficult dialogues that arise in multicultural clinical contexts. For example, Sue et al. (2019) propose that the therapist learn microinterventions for those patients harmed or traumatized by culture wars, interventions “that validate the lived experience of people from marginalized groups; communicate to them their value as a person; affirm their racial or group identity; and offer support, encouragement, and also reassurance that they are “not alone” (Sue et al., 2019, p. 134).
Empathy—the capacity to accurately see the other—is one of the first victims of a group that is insufficiently held. Hopson (2024) suggests that supporting the development or restoration of empathy may involve the group therapist in a more active way within the group. Strategies may include: Inviting group members across differences to imagine being in the position of the other and articulate what that may be like; rearranging the seating in the group to place people in closer proximity to the other; interpreting the split within a group member: ‘I wonder if a part of you resonates with what at the same time feels alien to you?’ Other technical skills have been suggested in the recent literature to affirm the value of those who have been subject to microaggressions in the group and to help those who have enacted these prejudicial stances understand the consequences of their behavior and their defenses about not seeing the harm caused (Miles et al., 2021; Miserocchi & Leit, 2024). The effort here is to arouse in the group the nascent capacities for human connection across differences and to come to the belief that such work is freeing and fulfilling for all the group members.
Importantly, as Kaklauskas and Nettles (2020) remind us, the processing of cultural differences needs to be fully integrated into the overall clinical work of the group, not considered an add-on. And in that spirit, as they write, the therapist’s well-honed clinical skills and therapeutic attitude of “support, validation, and exploration” will deepen the work and encourage the members to increase their support and understanding of one another’s experience, both intrapsychic and psychosocial.
Summary
- Group process generally refers to the more covert emotional, relational, and defensive needs of the group participants that underly and motivate their overt behaviors.
- The therapist needs to be able to distinguish processes that are work–oriented and in the service of task achievement from those that resist, avoid, or subvert the rational work of the group. The therapist should appreciate that containing and working through destructive forces (in the group, the context of the group, or in the group leader) holds the possibility for creative growth and therapeutic change.
- While process illumination has always been a core part of the psychological work in those groups that are exploratory, unstructured, or psychodynamic in orientation, increasingly even structured group models, such as cognitive behavioral therapy, are acknowledging the importance of monitoring group process to help the group stay on task.
- Traditionally, group processes have been conceptualized and monitored in three core ways: a) work-oriented processes, such as those forces that foster a sense of cohesion and shared commitment and valuing of the group and its work; b) transference dynamics in which early self-other schemas and templates are projected into and onto the group; and c) group level regressive dynamics, such as splitting into dysfunctional subgroups and the emergence of scapegoating.
- Increasingly, conceptualizations of group process are incorporating a multicultural perspective where group events, themes, and patterns are seen as reflections of cultural clashes and tensions of the larger societal context in which the group is embedded.
Therapist Interventions
Defining The Group Therapist Role
What the therapist does in the group, how the therapist’s work role is conceptualized, and how to best intervene at any one moment, from silence and deep listening to deep interpretation of underlying dynamics in the group, is determined to a large degree by the theoretical orientation of the therapist. That is, the therapist’s theories of therapeutic change will shape what group phenomena are the appropriate subject of attention and exploration, the ways these phenomena are conceptualized (e.g., whether tensions in the group derive from pathogenic beliefs, negative transference reactions or sociocultural differences), and thoughts about what interventions will effect change in a healthy direction. For example, Yalom and Leszcz (2020), in their process-oriented interpersonal group work identify the multifaceted work of the therapist as including the establishing and facilitating the exploration of here-and-now process, managing transference, and providing transparency. They further posit that group leaders need to monitor and manage the boundaries of the group, build a therapeutic group culture, and shape norms in the service of therapeutic work such as encouraging group member self-disclosure. Kivlighan and Chapman (2018) place greater emphasis on the importance exploring group phenomena and choosing interventions within a multicultural framework. They note that group is a place where multiple identities exist and manifest, and that group therapists have opportunities to increase cultural awareness, reduce bias, and facilitate social change within their group members. Further, they posit that a therapist’s ability to utilize cultural humility, cultural comfort, and seek cultural opportunities leaves them more prepared to create inclusive and affirming group spaces, reduce experiences of oppression and social inequalities, role model these behaviors for the group early in its development, and better manage cultural impasses as the group matures.
Creating Safety
A therapist’s interventions are guided not only by specific theories of therapeutic change but also by transtheoretical principles, such as the need to create and maintain a sense of safety. Group members must feel safe to fully engage in the therapeutic process and benefit from group psychotherapy. Therefore, establishing safety is a critical task for the group leader, particularly in the early formative stages of group development (Rutan et al., 2020).
A safe group environment allows clients to explore their internal and interpersonal experiences, gain insight into their thoughts, behaviors, needs, and motivations, and navigate the process of giving and receiving feedback without feeling overwhelmed, threatened, or devalued (Greene et al., 2020). Importantly, the therapist must serve as a container for the intense emotions that can emerge in group interactions. This involves remaining empathically attuned to members’ emotional expressions while modulating their own responses in a way that supports affect regulation. Reinforcing therapeutic values and norms, such as inquisitiveness, curiosity, and attunement, helps foster a sense of safety and optimism within the group. When members trust that differences within the group can be accepted, they are more likely to engage meaningfully in the therapeutic process.
To create an environment that promotes safety, therapists need to cultivate their own self-awareness of psychological issues that trigger defensiveness or countertransference reactions, as well as of processes of identity development, power, and marginalization, to minimize colluding in untoward group processes such as scapegoating or stereotyping. That is, therapists need to acquire their capacity to explore their own psychological and sociocultural development, including their training experiences, to appreciate their blind spots, obstacles to empathic attunement, and potentials for entering into harmful enactment. Further, therapists should be mindful of the theories and interventions they were trained to use in their work and be curious about what informed their development to avoid replicating oppressive dynamics that have historically existed in the mental health field (Ribeiro, 2020).
As highlighted throughout these guidelines, therapy groups often mirror the social and cultural dynamics that group facilitators and members experience outside of the group (Yalom & Lesczc, 2020). To foster safety in group, group therapists must develop cultural competence, including the awareness of historical and current oppressive dynamics against historically marginalized communities. Awareness and understanding of the ways oppression and marginalization manifest within the group allows therapists to avoid engaging in their own enactments (Abernethy, 2024; AGPA, 2023 Ribeiro, 2020).
A therapist’s willingness to model openness and vulnerability around their own salient identities and inviting group members to do the same, as it feels meaningful and salient to them, can help make group members trust that the group is a space where all identities can be welcome and seen. It is important to note that some group members may need additional support on how to hold space for their own identities and values when these principles feel different from others in the group. This again presents opportunities for clinicians to role model how to create co-existing space for different life experiences in a group setting.
Shaping and Implementing Group Norms
Implementing and reinforcing therapeutic group norms and values is another essential therapist task. Group norms guide the interactions of the group and help therapists create a therapeutic culture that enables change (Yalom & Leszcz, 2020). These norms can be understood as aspirational goals that guide how members are to be and relate in the group.
Group composition (e.g., presenting concerns) and members’ identities influence what norms feel safe for group members. Further, Kivlighan and Chapman (2018) posit that group norms should be established in a culturally sensitive manner. Cultural factors, such as relationships to authority figures, level of comfort with self-disclosure, and emotional expression, impact the way group members engage with groups and their commitment to the group goals (Ribeiro, 2020; Yalom & Leszcz, 2020). That is, group norms that the therapist considers important to the group process might not always fit a client’s cultural context and identities and may need to be adapted. For instance, as discussed in Chapter 4, time orientation varies across cultures (Sue et al., 2019). As a result, a group member arriving late to sessions might not be indicative of unwillingness to adhere to group norms or be symptomatic of underlying concerns, but rather a different relationship to the passing of time. Furthermore, a group’s expectation for self-disclosure or providing feedback might be difficult to meet for members coming from certain cultural backgrounds or who have had to hide parts of their identity due to systemic oppression. It is thus important for therapists to understand, in their efforts to establish and reinforce group norms, that clients’ participation in group, as well as their engagement with the group leader and other group members, is influenced by their presenting concerns, identity, cultural background, and experience. Explicitly addressing identity, history, and current sociocultural experiences can allow group facilitators to avoid over pathologizing behaviors that are culturally appropriate while helping clients connect with the group in ways that resonate with their experience and identity. Chapter 4 addresses the importance to discuss such factors before the group begins in order to start group meetings with a frame already established.
Group norms should be created in collaboration between the group leader and group members (Yalom & Leszcz, 2020). Group leaders can help group members understand what norms can facilitate the therapeutic group process (Yalom & Leszcz, 2020) and can also model the norms discussed, but they also need to be sensitive to how members experience these norms. Flexibility around ways that members can engage with group norms will provide space for them to participate authentically. Further, therapists and group members can openly explore needs that would help enhance safety and accessibility (AGPA, 2023). For instance, when discussing group participation and engagement, group facilitators should make space for diverse ways to engage with the group. This could include discussing nonverbal ways to communicate the need for support when overwhelmed by emotional reactions to group content or flexibility with in-person attendance for group members experiencing chronic health issues, etc.
Alliance
As discussed in previous chapters, group therapists must understand the importance of a positive therapeutic alliance between groups members, the group, and the therapist to ensure successful work in group (Alldredge et al., 2021; Bernard et al., 2008; Burlingame et al., 2004; Zilcha-Mano, 2017). Consequently, group leaders should attend to members’ commitment to the goals and work of the group, as well as to the quality of the bonds within the membership and between the members and the group leader. If there is any indication that a facet of alliance is not present, group leaders should address it with the group.
Therapists can promote a positive therapeutic alliance between the group members and themselves by demonstrating that they are ready to hold the group’s emotional experiences and that they are actively listening to group members’ disclosures. Reflecting on what group members share out loud with compassion and curiosity (e.g., asking questions or inviting members to expand), using their own body language to show their engagement (e.g., nodding, use of facial expressions), checking that they are on track when offering interpretations of what group members shared, or introducing coping skills or psychoeducation are positive ways for therapists’ to show their commitment to the group, its members, and goals (Rutan et al., 2020). Keeping the group on task and holding the frame established with clients at the beginning of group are also important ways to create trust and help clients know that the therapist is reliable.
For a group to be successful, members need to trust that other members are invested in their success and growth. Group leaders can model the care and respect they hope members will display for each other (Bernard et al., 2008). Encouraging members to engage with each other with vulnerability and empathy can help build strong alliances between members. For instance, group members can encourage each other by sharing insight or discussing ways in which their experiences are similar (Rutan et al., 2020). Members’ ability to do so will increase their willingness to use self-disclosure and to feel safe in the group. Strong alliances between members also increase the likelihood of committing to the work of the group and providing each other feedback (Rutan et al., 2020).
Group leaders need to be aware that visible and invisible diversity could affect alliance between group members and therapist, as well as between members (Chen et al., 2008). This is not only explained by differences in experiences, but also by larger social power structures and their impacts on each of us. Use of self-disclosure about the therapist’s own identities and how they might differ from those of group members can be particularly important in strengthening alliance (PettyJohn et al., 2019) as it demonstrates awareness of differences in power and willingness to use that awareness to understand client experiences. Therapists can also use measures to assess alliance in their groups and discuss results with the group. For instance, the Working Alliance Inventory (WAI) (Horvarth & Greenburg, 1989) and the Group Climate Questionnaire (GCQ) (MacKenzie, 1983) are two self-report measures that can be completed by group members as they progress through the stages of the group. When alliance may be impacted by clients’ and therapist’s identity, being flexible and creative in finding ways to strengthen the relationships of the group can be helpful. Miles et al. (2023) review and recommend additional process measures that compliment leaders’ clinical judgement and may provide guidance for addressing cultural issues.
Providing, Receiving, and Mediating Feedback
Most models of group therapy, even structured CBT groups, provide therapeutic opportunities for learning about one’s interpersonal behaviors, needs and emotions, how they originated, what purposes they served, and how others in the group experience them. Group therapy is a powerful tool in helping individuals develop insight into their own behavior and reactions, as well as into their impact on others (Bernard et al., 2008). This particular type of insight is possible through giving and receiving feedback from group leaders and other group members. Research has shown that feedback in group psychotherapy increases insight into one’s own behavior, as well as increases motivation for change, willingness to take interpersonal risks, overall satisfaction with the group experience, and reinforces behavioral change (Chen et al., 2008; Kivlighan et al., 2020; Morran et al., 2004). Through facilitating safety, reinforcing culturally sensitive and affirming norms, and modeling the giving and receiving of feedback, therapists can create an environment that facilitates this process.
While research and various theories emphasize the importance of feedback, past studies have also suggested that group members seemed to perceive giving positive feedback as more acceptable than providing more negative feedback (Kivlighan et al., 2020). However, it appears that a balance of positive and negative feedback affords more benefits for group members (Kivlighan et al., 2020). The sequence in which the feedback is given also appears to matter. Therapists should be aware that providing more positive feedback at the beginning of group is conducive to more progress (Morran et al., 2004). By increasing group cohesion (Chen et al., 2008), early positive feedback exchanges expand a group’s ability to provide meaningful feedback, including more negative feedback later. In middle and later stages of the group, negative or corrective feedback is often received better when positive feedback is provided right before and after, and when the feedback and focused on observable behaviors (Morran et al., 2004). Being aware of this sequence will help therapists foster more openness to feedback in the group.
More generally, it is important for the therapist to create a group environment that feels safe enough for members to take the interpersonal risks associated with giving and receiving feedback. This can be done by being mindful of how cultural norms influence one’s willingness to give/receive feedback (Chen et al., 2008). Helping clients process the feedback they have just received is essential to understand their present experience and solidify the feedback. Focusing on the here-and-now when feedback is provided also helps group members engage in the group in a way that resonates with their own individual experience (Chen et al., 2008).
Using the Here-and-Now
Most theories of group psychotherapy, even structured CBT groups (Greene, 2024), emphasize the utility of the therapist’s encouraging the group members in exploring here-and-now processes in the group (Yalom & Leszcz, 2020). It is important for group therapists to be able to differentiate the content of what is shared by group members (i.e., the overt words and behaviors of the members) and the process involving the here-and-now (i.e., the underlying dynamic relationships that are being enacted in the group; (Greene, 2024). The therapist can promote the exploration of here-and-now process by inviting members to share their own interpersonal needs and emotions in the moment and their reactions to the group-as-a-whole and the other members—work that encourages an inquisitiveness both about one’s own inner world and about who the others are in the group. Therapists can model such inquisitiveness, especially at the early stages of group, by reflecting on what they hear group members share out loud, by asking questions about the members’ internal experiences, by inviting members to slow down and elaborate, or by noting observations they are making in the group.
Therapist Transparency and Use of Self
One of the controversial matters pertaining to the group therapist’s role and technique is that of therapist transparency and how the therapist uses self in the treatment (Yalom and Leszcz, 2020). What should therapists reveal about themselves, and what should they keep private (Bernard et al., 2008)? There are two generally accepted guiding principles: (1) therapists should not reveal anything that they are uncomfortable sharing about themselves although therapists have different thresholds for what they share; and (2) the only legitimate rationale for the therapist’s personal disclosure is the thought that it will facilitate the work of the group at that moment in time.
Sometimes therapist self-disclosure involves telling group members about experiences outside the group, though this decision should be based on the hypothesis that such revelations will illuminate some aspect of the current group process. At other times, a therapist self-disclosure will involve describing their experience of a group member. Feedback about the group member’s behavior and interpersonal impact can be very useful, particularly if it models for the group the process of feedback and is delivered in a way that is constructive without shaming or blaming the client. If the therapist and member in question have a positive therapeutic alliance, and the therapist offers the feedback in a way that indicates interest and concern rather than anger and a wish to be hurtful, this kind of intervention can be enormously helpful, not only for the individual in question but for the group-as-a-whole.
Yalom and Leszcz (2020) label therapist transparency as an essential intervention, where clinicians are able to respond to members, share their feelings, acknowledge or refute motives or feelings attributed to them, and self-reflect on their own inner world, including blind spots and vulnerabilities. PettyJohn and colleagues (2019) also note how important self-disclosure can be when working with diverse clients. Each therapist is tasked with determining the pace, degrees, and nature of their transparency as balanced with the various other tasks that fall in their roles.
Of course, group therapists reveal things about themselves in a number of ways besides what they verbalize, including body posture, voice inflection, what they wear, how they set up their offices, how they handle fees and other arrangements, and how they interact with the array of people in the group. It is important for group therapists to remain mindful and curious about their metacommunications. For example, a therapist’s decision to address or not to address a microaggression in the group can convey information about the therapist’s values, their privileges, or how they handle conflict. Group therapists are more exposed than individual therapists because they interact with a variety of people, who elicit different aspects of their identity, simultaneously and in front of everyone in the group.
Addressing Group Boundary Violations
Inevitably, group norms will be violated by group members throughout the group process. Boundary violations can range from behaviors outside of the group (e.g., failure to pay for services) to inside of the group (e.g., aggression, inappropriate touch). Addressing violations is another essential task of the leader as the leader’s response can reestablish safety (Greene & Kaklauskas, 2020). While some issues may need to be addressed outside of the group with an individual client (e.g., failure to pay for services), others will need to be addressed in the group. Group therapists should approach the violation with curiosity and explore what is behind crossing group boundaries. Whether the violation is an attempt to communicate a need to the group or an indication of how the norms do not fit a member’s experience, taking the opportunity to discuss the violation in the here-and-now, as quickly as possible, can help the group move toward its goals (Rutan et al., 2020).
Therapists have a responsibility to identify how to work towards resolution following a norm violation. To do so, they must be able to identify the type of harm that was caused to the group and to individual members. The therapist’s primary responsibility is to maintain the structure of the group and reinforce boundaries that promote safety. While it is important to be able to work through the challenges with the group, there will be times when members might be asked to leave a group to protect other members and preserve the safety of the group (Rutan et al., 2020). In such cases, therapists should always provide space for the member to understand the decision and provide alternative treatment referrals.
Addressing and Repairing Ruptures
Ruptures in group therapy are also inevitable and can be difficult to manage as they can occur at three levels of interaction (singularly or simultaneously): member-to-member; member-to-group; and member-to-therapist. Therapy ruptures can be defined as a change in the therapeutic relationship leading to a diminished commitment to and engagement in working on the shared goals and tasks of the group (Tasca & Marmarosh, 2023). Group therapists’ effective management of ruptures that occur in the group are also essential interventions in maintaining a therapeutic group culture and member therapeutic outcomes. While ruptures in the group can be essential to experience and work through to eventually enhance cohesion (Yalom & Leszcz, 2020), some ruptures may cause significant harm and need immediate intervention. This has been even more notable with the presence of cultural ruptures in our ever-diversifying group spaces.
The recent literature provides interventions that therapists can use when ruptures, both cultural ruptures and pathological interpersonal processes, occur in group. For example, in their work on microaggressions, Miles and colleagues (2021) suggest that the therapist help the group through the difficult conversation of exploring the rupture, provide support to those who were harmed, and help those who committed the harm to explore and gain greater awareness of the harm induced without instilling shame or blame. This can be done by naming the microaggression (or other type of rupture), illuminating the process underlying it, educating the group member who perpetrated it and increasing their affective tolerance, and practicing receiving feedback by avoiding shame but fostering accountability. Finally, with respect to any kind of rupture arising in the group process, the therapist can work to help create a corrective emotional experience (Miles et al., 2021) for the group, involving reinforcing increased containment, understanding, compassion, and tolerance for the differences between self and other.
Co-leadership relationship
Co-leadership is a structural arrangement widely used by therapists practicing group psychotherapy across settings of care (Yalom & Leszcz, 2020). Specifically, co-leadership is often utilized in training settings where a more experienced therapist leads a group with a therapist-in-training. While it is thought to afford some advantages to the group therapy process, its added complexity also brings challenges that need to be faced.
The limited available clinical literature on co-leadership does posit several benefits to leading a group with another therapist rather than on one’s own, such as the opportunity to: 1) model healthy interpersonal behavior for group members, including the negotiating of interpersonal differences (around power, authority, style); 2) have a second set of observations and formulations about what is going on in the group that either support or provide an alternative perspective for the therapist; and 3) feeling more supported and connected through collaborating and thus reducing therapist anxiety.
While these potential benefits are significant, potential challenges and disadvantages should also be considered when deciding whether to lead a group alone or with a co-leader. A core challenge to co-leadership is how differences between the two therapists will be negotiated. Therapists with different value systems, theoretical approaches to therapy, therapeutic styles, and cultural identities might experience conflict and competition as co-leaders. Who speaks when, who will have a voice at any one moment, and whose voice will be heard? These differences between the therapists can also evoke differential affective reactions in the group-as-a-whole or in different members as happens, for example, when the co-therapist team is split by the group into a good therapist-bad therapist configuration. The key here is that the differences between the co-leaders—those they bring into the arrangement and those that are projected on to them by the group members—need to be contained and explored as part of the work of the group. This work needs to occur before the start of the group, during the group sessions, and in debriefings after the group sessions.
The core of what makes a co-leadership successful is the therapists’ commitment to: understanding and staying engaged in the therapeutic process; forming a collaborative team where co-leaders respect each other’s perspectives and ideas; demonstrating an openness to explore their relationship and tension when it arises; not assuming that their co-leader knows their plans and ideas but communicates them clearly; agreeing on how to share leadership roles and tasks; and agreeing on the group structure, group culture, goals, and mechanisms of change. Successful co-leaders can work through conflicts and are willing to receive personal supervision to explore their own role in the co-leadership.
Summary
- While the therapist’s work role is determined to a large degree by the theoretical orientations that the therapist holds allegiance to, other interventions are guided by more universal concerns to create a safe work-oriented group climate.
- Group therapists must create groups that are safe for clients with diverse presenting concerns, histories, and backgrounds.
- In addition to creating safety, group leaders should ensure that their interventions foster a positive alliance between themselves and the group, as well as between group members.
- Group leaders can model sharing feedback and being open to receiving feedback to support group members in becoming more comfortable with it.
- An important role of the group leader involves keeping the group on task, which can be done by utilizing the here-and-now.
- If co-leading a group, group facilitators should be mindful of the way they engage with each other and with the group.
The Ethical Practice of Group Psychotherapy
These guidelines borrow from ethical standards promulgated by national practice and professional organizations, such as the American Counseling Association (2014), American Psychological Association (2017), National Association of Social Workers (2021) and the Association for Marriage and Family Therapists (2015), as well as the American Group Psychotherapy Association and International Board for the Certification of Groups Psychotherapists (2002), and interpret, expand, and apply them to the practice of group psychotherapy. When in doubt, these guidelines should serve as a guide and readers should consult and utilize the ethics codes that correspond with their professional identity and licensure.
Ethical Decision Making
Clinical challenges inevitably arise in the therapy group and knowing the process of ethical decision making is important to sort out the course of action that optimizes the most good, minimizes harm, and safeguards autonomy for the group members. One of the most thorough processes of ethical decision making has been outlined by Pope et al. (2021). They propose a rigorous 15-step process that includes: a detailed specification of the problem or concern, a comprehensive accounting of everyone who might be impacted and considerations of what the impacts might be; a review of the current theoretical and empirical literature, as well as the relevant legal and ethical standards; and, importantly, an exploration of how the therapist’s self may be influencing judgment and decision making. Regarding this last point, they recommend consulting with experts and colleagues in the field.
When encountering an ethical dilemma, the prudent group psychotherapist ensures their decisions follow each one of the listed steps. It is important to recognize that ethical decision making is not always clearcut and is at times nuanced. In those situations, the inherent values of the various ethics codes—the guiding principles—assist group therapists in remaining ethical to their respective fields and to the clients they serve. Two of the consistent values across professional ethics is that of beneficence (to benefit those we treat) and nonmaleficence (to do no harm (American Psychological Association, 2017). These guiding principles must take precedence in any decision about what to do to protect those we serve.
The following ethical dilemmas and challenges are ones that the group psychotherapist is likely to face. While real-life clinical situations will be unique, understanding these potential dilemmas and challenges will be useful in supporting therapists in making ethical decisions.
Confidentiality
Confidentiality in group psychotherapy refers to the ethical and/or legal obligation of a therapist to protect the privacy of a group member’s personal and sensitive information by not disclosing any information about the member to third parties without the member’s consent, except in certain circumstances where there is a legal or ethical obligation to do so, such as in cases of suspected child or elder abuse or harm to self or others. Confidentiality is a key prerequisite of the therapeutic enterprise, as it helps to establish trust and allows clients to feel safe and comfortable sharing their thoughts and feelings with their therapist and with others in the group.
Within individual psychotherapy, privileged information is relatively easy to maintain (Adi & Mathbout, 2018). However, in the case of group psychotherapy, confidentiality is more difficult to maintain and cannot be guaranteed. Some states and jurisdictions have a “third-party rule” that states that any information disclosed where a third party is privy to it cannot be considered privileged or private information. Simply stated, group therapy members in these jurisdictions are not legally bound to maintain the confidentiality of what is disclosed in the group. In other states, specific statutes specify that information about other group members that is disclosed outside of the therapy group can be prosecuted under the local statute. Group therapists are responsible for being familiar with the laws of their local jurisdiction and for each jurisdiction in which they practice and are licensed. In addition, the limits of confidentiality should be clearly outlined in the informed consent documentation, reviewed during the group preparation process individually, and at minimum, reviewed again during the initial group meeting and whenever a new member joins the group. Specific implications or consequences should be stated regarding the limits of confidentiality or should confidentiality be violated.
It is important for group therapists to understand that emphasizing the importance of confidentiality and clarifying its limits in each group therapy situation serves to facilitate trust, thus allowing for more personal and open communications in the group, but also highlights the potential for harm should confidentiality be broken, whether or not it is legally mandated. Breaches of confidentiality can lead to serious real-world consequences, such as loss of employment, marriage, and social status (Roback et al., 1992) and can disrupt treatment. What happens in group, stays in group is a good mantra for the therapist to keep in mind, not only for traditional therapy groups but also, as discussed in Chapter 11, online groups.
Multiple Relationships
Multiple relationships (or dual relationships) occur when a therapist is engaged in a professional role with a person and “at the same time is in another role with the same person, at the same time is in a relationship with a person closely associated with or related to the person with whom the psychologist has the professional relationship, or promises to enter into another relationship in the future with the person or a person closely associated with or related to the person” (American Psychological Association, 2017). Because of the potential to disrupt the treatment process, multiple relationships should be avoided by the group therapist.
As discussed in Chapter 10, the practice of combined therapy, as in conducting individual and group therapies with the same client, poses ethical and clinical challenges. How, when, and why information gathered in one modality can be brought into the other modality needs to be carefully worked through and negotiated with the client in the preparation phase so as not to violate the client’s right to privacy and confidentiality and create disruptive experiences. Depending how the boundaries between the modalities are managed, this particular kind of dual relationship can either enhance or hinder therapeutic progress. The group therapist practicing combined therapy needs to keep in mind the specific and unique goals and anticipated outcomes within both modalities and how they two modalities are expected to relate to each other.
Group Leader Competence
Competence is an ethical standard maintained by all licensed mental health professionals in their field. The practice of group psychotherapy is a specialty that requires specialized training and the attainment of unique skill sets, as well as a minimum of 20 hours of on-going group psychotherapy continuing education every two years (AGPA, 2002).
Core competencies are considered essential for the successful functioning of a group therapist (Barlow, 2012; 2013). These competencies have traditionally been separated into foundational competencies and functional competencies. Foundational competencies refer to “knowledge, skills, attitudes, and values that make up the base or foundation from which professional psychologists operate” (Barlow, 2012, p. 444). When applied to the group context, foundational competencies include reflecting on oneself as a group leader, being involved in research, engaging in group level relationships, being aware of diversity present in the group setting, understanding the ethical and legal standards surrounding group psychotherapy, and appropriately interacting with all members of a group (Barlow, 2012, 2013). Functional competencies, defined as “those actions or functions put to a particular purpose by professional psychologists” (Barlow, 2012, p. 446), include assessment strategies, group formulation and conceptualization, group interventions, group consultation, group research and evaluation, group supervision and teaching, and group advocacy (Barlow, 2012, 2013). These foundational and functional competencies can be acquired through many different avenues, including formal and informal education, continuing education, workshops and mentorship. The ethical group therapist continuously assesses mastery of these competencies and seeks out additional training and supervision when necessary.
Reducing negative outcomes
The heart of ethical practice is preventing harm for the clients we serve. However, within the complex setting of a therapy group, significant harm may occur through the actions of the group members. While the group therapist is responsible for reinforcing therapeutic norms and values and creating a culture of safety and respect, all of which serve to minimize harm, the leader is unable to control the actions of any of the group members. Even the most competent of group therapists cannot prevent the emergence of damaging incidents, such as a member’s boundary violations or destructive group forces of scapegoating, enactments of biases and oppression, empathic ruptures and misattunements, or entrenched defenses and resistances to work (Greene & Kaklauskas, 2020; Griner et al., 2022; Leszcz, 2018). Conflict and aggression are inevitable in the group; destructive and damaging processes can occur in the relationships of member-to-member, member-to-group, and member-to-therapist (Tasca & Marmarosh, 2023). As such, the therapeutic strategy or intervention used to respond may need to be specific to the level at which the rupture occurred (Garceau et al., 2021; Tasca & Marmarosh, 2023).
The resulting damage and hurt can disrupt treatment for the individual group member and the group-as-a-whole, manifested as worsening of presenting symptoms, appearance of new symptoms, a loss of hope or trust in the therapist or therapy process, or drop-outs. It is incumbent upon the group therapist to try to contain the destructive forces through such interventions as restoring empathic connection and helping the group explore, identify, and understand the defensive aims that anti-therapeutic interactions serve (Spotnitz, 1981; Yalom & Leszcz, 2020; Zeisel, 2012). If the leader and the group cannot adequately contain and work through these dynamics, negative outcomes are increasingly likely.
Staying in the here-and-now can help group members understand their impact on others and their own internal experiences and reactions in deeper and more nuanced ways. However, while exploration of difficult events and dynamics is an important part of therapeutic work, group facilitators will at times have to actively interrupt behaviors or processes causing harm to maintain safety and the therapeutic frame (Greene & Kaklauskas, 2020). Care must be exercised, along with demonstrative skill such that, in the process of attending to aggression and conflict, individual group members have an opportunity to understand their impact, while the experiences and reactions of those impacted are honored and respected by the group. Exploration of ruptures within the group provides an opportunity for individual clients to understand patterns of behaviors and enactments that reflect their interpersonal experiences outside of the group. The process of exploring the harms should also include curiosity and ideas about how to repair. Therapists can encourage clients to take responsibility and gain insight with compassion to create a reparative emotional experience for all involved (Tasca & Marmarosh, 2023). When ruptures happen at the therapist-client level, therapists can model taking responsibility and creating change without shame by directly addressing the rupture with the group and repairing the harm.
Of particular significance is the management of microaggressions and macroaggressions to individuals who hold marginalized identities. Various tensions and forms of oppression existing in larger society are likely to enter the group space and the group can create an environment in which these dynamics may be carefully addressed and productively dismantled. Care and attunement, along with acknowledgement of personal unconscious biases, must be taken by the group therapist to recognize these processes within group psychotherapy and to manage them, which encourages repair and cohesion (Miles et al., 2021).
Leadership issues
Experience, ongoing training, continuing education, and supervision can help group leaders maintain or improve levels of competence and reduce the risk of creating, contributing to, or failing to adequately address potential harm. Ongoing access to one’s own internal world helps group therapist remain mindful of what they bring into the therapy room. For instance, while self-disclosure can be a helpful tool in therapy, group leaders should be mindful of the reasons why they decide to engage in personal disclosures with their groups. Leaders who are struggling emotionally may be more apt to break boundaries they would traditionally hold, and the oft repeated encouragement towards self-care is also care for one’s group clients (Greene & Kaklauskas, 2020; Norcross & VandenBos, 2018). Leading a psychotherapy group is inevitably challenging given the projections, implicit invitations, and covert dynamics aimed at the therapist, and personal therapy is considered a way of more deeply understanding oneself and helping to sort out what at any moment is projected onto the leader and what derives from the leader’s own internal world (Yalom & Leszcz, 2020).
Boundaries and ethical violations
As discussed in previous chapters of these guidelines, violations of the therapeutic frame can disrupt the work of the group. While group therapists should remain flexible to respond to the unique needs of their group, holding the frame and reinforcing therapeutic norms and values are important in maintaining safety (Rutan et al., 2020). However, boundary and ethical violations can also come from the leader. Group therapists are exposed to a dizzying array of dynamics, which can at times become difficult to hold and contain. Finding and sustaining self-care is an essential part of our profession, as well as seeking consultation when confronted with challenging group dynamics. While sharing one’s work can feel vulnerable, retreating to isolation and defensiveness when under professional stress is in no one’s best interest.
Group leadership provides endless opportunities for therapists to mature and grow as both people and professionals. Enhancing awareness of our own countertransference tendencies and finding constructive ways to work with our group-based challenges is important in providing good care to clients. As part of this process, group leaders also need to analyze their own socio-cultural positions to create therapeutic spaces that are effective for the needs of diverse populations, particularly those who have been historically marginalized in medical and mental-health settings. Historically marginalized populations access therapy less than those from dominant cultures, and often their experiences are not one of healing but of further marginalization (Jimenez et al., 2022). Group leaders with culturally dominant identities need to integrate these issues into their case conceptualization and therapeutic work and not steer away from diversity discussions in their groups or minimize the impact of power and oppression within their groups (Miles et al., 2021; Zaharopoulos & Chen, 2018). Further, group facilitators should be aware of ways in which sociocultural enactments may manifest in their group so they are able to interrupt them and explore them with the group. Regularly examining the interaction in our groups from the perspectives of power, privilege, and oppression is an essential lens to avoid merely recreating oppressive social dynamics in groups (Chang-Caffaro & Caffaro, 2021; Yeo & Torres-Harding, 2021).
Ongoing feedback from members
Therapists should regularly check in with the group members about the impact of the group towards their goals, as well as any thoughts they have about the processes occurring in the group (Yalom & Leszcz, 2020). This relational qualitative approach is very helpful in building collaboration, tracking progress and treatment planning. Over the last several decades, increasing interest and research has been conducted on practice-based evidence (PBE), on the use of standardized measures to compliment clinicians’ perspectives (Castonguay, 2021). Often, these measures assess symptoms, as well as alliance with the therapist. In group psychotherapy, these measures often assess aspects of the group process, group cohesion, and the emotional bonds within the membership and between the members and the leaders (Burlingame & Jensen, 2017; Whittingham et al., 2023). Research has shown that clinical judgment can sometimes miss information that may show up on an instrument, and this is particularly vital to capture sociocultural enactments and ruptures that may not come forth during a group discussion but deeply impact members progress, alliance with the leader(s), relationship between co-leaders, and trust in the group (Burlingame et al., 2002; Chang-Caffaro & Caffaro, 2021; Kivlighan et al., 2019). Incorporating practice-based evidence tools has shown positive impact on outcomes (Burlingame & Strauss, 2021). The Group Psychotherapy Assessment and Practice: A Measurement-Based Care Approach (Macnair-Semands & Whittingham, 2023) from the AGPA Group Therapy Training and Practice Series provides important information to support group leaders’ in assessing their members’ experience.
Conclusion
The examples outlined in this section are not exhaustive and should not be viewed as such. The ethical practice of group psychotherapy remains the responsibility of the group therapy practitioner to remain informed of the ethics code for their profession, the legal and ethical code mandated by their jurisdiction of practice, as well as the current literature on best practices within the field of group psychotherapy. When in doubt, the ethical group therapist engages in supervision and consultation to help navigate difficult situations, maintain professional integrity, and to prevent undue harm to the clients we serve.
Summary
- Group therapists should be familiar with their respective ethics codes, as well as with the pertinent laws and regulations in the jurisdictions in which they practice.
- Group therapists should strive to preserve the confidentiality of their group members, educate them about limits to their confidentiality, as well as about ways to protect each other’s privacy and the risks associated with breaching those guiding principles.
- Group therapists should obtain specialized training and keep their training up to date to ensure that they are competent in providing the services they practice.
- Group therapists should also strive to mitigate negative outcomes by increasing their awareness of their own internal world, reinforcing the group frame, and addressing boundary violations when they occur.
Termination
The word ‘terminate’ derives from the Latin verb termināre, which means to set a boundary. This definition captures one meaning of termination from group psychotherapy—ending one’s membership in a group. But termination is not just the overt act of leave-taking, it also is about the process of leaving, a process that encompasses: (a) the experiences of the departing member, the remaining members, and the therapist as a member’s exits from the group; and (b) the subsequent reactions of the therapist and continuing members following the departure. Because the second meaning of termination has such significant implications for what therapist interventions are likely to benefit members during this period, it is the major focus of this section. However, the first meaning, which is connected to practice management issues, is addressed in the latter part of the paper.
Types of Terminations
Ending experiences for all involved will be shaped by whether the termination occurs in a closed-ended versus open-ended group (Rutan et al., 2014) and whether it is planned versus unplanned (Klein, 1996). In a close-ended and time-limited group, all members begin in the same session and end in the same session. In such a framework, group members know at the outset when they will experience their last session, recognize that they will share participation in this process, and potentially keep termination in mind through the duration of the group. In an open-ended group, members depart from the group at different times, ideally leaving when the person’s therapeutic goals have been accomplished. In this structure, the group members must contend not only with the loss of the member but also with the uncertainty of how the group will be altered by that member’s absence. Although, typically, open-ended groups entail individual departures, special factors, such as the therapist’s decision to retire, can result in all members of an open-ended group leaving at the same time. Likewise, in a close-ended group, a member might depart the group earlier than the expected date due to a variety of factors, an occurrence that invites a second important distinction—that between planned and unplanned terminations.
Planned terminations are those endings that ideally (a) occur once the member has made significant positive changes; and (b) provide the member and the group the opportunity to process the termination. The positive changes might correspond to the problem areas identified during the pre-group preparation, as well as additional problem areas that emerged over the course of the sessions (Rutan et al., 2014). At times, the member, others in the group, and the therapist might disagree about the client’s readiness for termination. In such a circumstance, the ethical principle of respect for autonomy demands that the member’s view be given considerable weight (Brabender & MacNair-Semands, 2022). The termination might be unilateral or mutual. In a mutual termination, the member incorporates the feedback of the therapist and other group members on readiness to leave, whereas a unilateral termination is made independently of other parties in the group and may reflect a weakness in the therapeutic alliance (da Silva et al., 2021). Unplanned endings do not afford members the opportunity to have a robust experience of termination with the departing member present. Many factors can lead to an unplanned termination, including those that are situational (i.e., a member relocates for work), individual (i.e, the therapist and member see the member as failing to benefit from group participation), or interpersonal (i.e., the member departs the group in reaction to a rupture with another member or the therapist).
In some cases, planned terminations can be interrupted. For example, the therapist or group members might so value the contribution of a given member to the group that the member is explicitly or implicitly discouraged from leaving (Yalom & Leszcz, 2020). Group psychotherapists need to be vigilant about a pressure to allow their own self-interest to dictate a termination-related decision. The terminating member of the group might also find the loss of the group resource so daunting as to cancel an intended departure from the group. Again, therapist alertness in relation such a dynamic allows for its exploration in the group.
Member Reactions to Termination as Opportunities for Growth
Termination evokes a wide range of emotional reactions in group members and the therapist. From the perspective of both leaving and remaining members, loss is a core aspect of the experience of termination. For the departing member, the loss is that of the relationships with the members, the therapist, and the group-as-a-whole. The remaining group members and the therapist lose not only their relationship with the departing member but also the predictability that comes with a known member and an ability to anticipate what they can expect from one another, even if these expectations are, at times, unmet. With each departure, the group becomes a new group, and the prior group is gone. The feelings that are dominant during this epoch of group life are those commonly associated with loss of relationship including, but not limited to, sadness, anger, disappointment, fear, and guilt. Intensifying these emotions is the power of termination to activate prior loss memories. Particularly salient are experiences associated with death insofar as the termination of a member has a permanent character. In contrast to the individual psychotherapy situation, the departed member cannot so easily return to the group and even if the member did, it would be a new group, one likely populated with new and old members and whatever unique dynamics emerge from this composition (Yalom & Leszcz, 2020). Mourning can occur well after a member has departed. Rutan (2021) describes a circumstance in a group meeting in which a member’s puzzling behavior in the session could be understood only once it was realized that the group was meeting on the same day a beloved group member had left a year prior. Group psychotherapists do well to look for not only short-term but also long-term loss reactions.
Unsurprisingly, members are motivated to avoid the pain of losing the group and other losses it might symbolize. Regression to a more primitive mode of functioning, a mode allowing members to bypass the important change that is occurring in their lives, is common (Zilberstein, 2008). Members’ motivation to avoid a loss experience is great given that it is often a difficulty in confronting loss that brings members into treatment (Piper et al., 1992). The regression exhibited by members can take different forms. Members might begin to show modes of interaction characteristic of their relating in the group’s earliest sessions or an intensification of the problems that brought them into treatment, patterns that might be protests against termination (Yalom & Leszcz, 2020). Groups employ more specific defenses to fend off aspects of their loss reaction. For example, members might idealize the group on one hand, to spare themselves from contending with disappointment in relation to whatever the group could not provide, or devalue the group on the other hand, to pretend that nothing of value is being lost (Brabender & Fallon, 2009).
Some termination reactions are specific to whether a member is departing from the group or remaining as another member departs. A common reaction of departing members is fearfulness about how they will fare once this resource is absent from their lives. Doubts about the progress they’ve made over their tenures in the group might also surface. These members, though, can and often do feel pride that they’ve reached a point of being able to terminate from treatment (Zilberstein, 2008). Members who remain in the group can easily feel apprehensive about their own progress, particularly if their tenure in the group matches that of the departing member, envious of the departing member (Bernard et al., 2008), and hope that they, too, will make the progress enabling their departure (Shapiro & Ginzberg, 2002).
Variation in Termination Phenomena
Although termination is evocative of a common set of reactions, groups and members within groups show variability in what reactions are most likely to be salient. Among the factors most likely to affect responses to termination, the following are likely to play a key role:
- Type of Termination—When terminations are planned, members nonetheless will contend with difficult reactions but will likely have the satisfaction of having the opportunity to explore their reactions fully. Planned terminations support a sense of order and safety in the group. In contrast, precipitous terminations are typically experienced as a disruption (Schneibel et al., 2017). In Fieldsteel’s (1990) words, “Group members may question the abilities and skills of the therapist, they may wonder where they have failed, and some may question the whole process of therapy” ( p. 29). Of course, the specific circumstances giving rise to the unplanned termination will make a difference in members’ responses. For example, an abrupt departure due to illness will likely evoke less of a sense of insecurity than one sparked by a rupture between the exiting member and other group members or the therapist. It is reasonable to suppose that members will see any current termination against the background of the history of terminations in the group and whether the unplanned termination is typical.
- A member’s termination experience is likely to be filtered through the lens of members’ culture. As Mangione et al. (2007) point out, how a culture regards loss and creates loss rituals is variable. For example, in a group in which a member leaves because of death following a brief illness, one member might feel that the person is forever gone, another that the person lives on albeit in a different form, and still another, that re-unification will occur with the departed member in the afterlife. Consider the following example:
Darika had been an energetic participant in the psychotherapy group where she dealt with issues pertaining to work. Specifically, she entered the group complaining of extreme anxiety in anticipating communicating with her supervisor at work. She made considerable strides in experiencing reduced anxiety before meetings with the supervisor, greater confidence in stating her needs, and enhanced skill in pointing out times when the supervisor’s perception of Darika’s productivity veered from the actual evidence. As the group approached its ending, Darika did not express feelings about the loss of the group even though she appeared to be concerned about the other members and how they would fare upon termination. She also was less verbally engaged than she had been in earlier sessions. In a prior session, the therapist had made a group-as-a-whole interpretation about avoidance of loss reactions. The members subsequently applied this interpretation to Darika and her seeming indifference to the group’s ending. Darika responded that she had had some very significant losses in her life, but she was consoled by her Hindu faith that enabled her to experience continuity in relationships even in the absence of face-to-face contact. She also talked about silence, a quiet reflective space, as a helpful resource to her in the presence of a loss.
This vignette illustrates that a member’s behaviors when facing loss and the feelings underpinning those behaviors are shaped by culture.
Members who have experienced a much lower level of marginalization and stigmatization in the psychotherapy group relative to society-at-large are likely to find the loss of the group particularly devastating (Burnes, 2020). These members will be prone to see the loss of the group as the erosion of their secure base, the well-spring of contentment, and capacity for adaptive action.
- Personality characteristics of the member influence how a member responds to endings (Joyce et al., 2007a). Marmarosh et al. (2013) point out that an individual’s loss-related reactions will be shaped by attachment style. For example, preoccupied individuals are more likely to become dysregulated when dealing with loss. Employing the Five Factor Model, Canuto et al. (2008) found that elderly outpatients with greater openness and agreeableness had more successful group terminations than individuals who showed lower levels of these personality traits.
- The maturity of the group also plays a role in reactions to termination. As the group matures, members are more able to attest to negative and positive aspects of group life (Brabender & Fallon, 2019). A more mature group, then, is likely to give expression to a richer experience of loss.
- When the psychotherapy group is embedded in a broader treatment program as is the case in inpatient and partial hospitals, as well as intensive outpatient units, the stance of the broader environment toward termination will permeate the group, enhancing or detracting from what termination work can occur (Brabender & Fallon, 2019; Kibel, 1981). Systems that recognize the importance of endings will support the group’s processing of the thematic material that emerges during this period of group life.
Therapeutic Opportunities within Termination
As Walsh (2007) notes, “Whether or not the ending of a clinical intervention is managed well can make the difference between successful and unsuccessful outcomes for the client and the professional.” (p. 5). The common themes emerging during this phase of group life create potential for further therapeutic work that can move members closer to their treatment goals. Members experiencing a loss within the here-and-now of the group affords them the chance to address loss in a more effective way than they have done in the past. Within the group, the ways in which members avoid having full experience of loss—one which acknowledges the range of feelings they have—can be identified. The fact that the loss is shared enables the group-as-a-whole to serve as a container for what members could find difficult to bear in isolation. The needed psychological work can vary from member to member. For example, an individual with a preoccupied attachment style is prone to become especially clinging and dysregulated and would benefit from understanding the meaning of these behaviors and recognizing the importance of establishing a support network outside the group. In contrast, the de-activating strategies used by the member with an avoidant style might be addressed by helping the members to recognize the fears that underpin the disengagement from emotions (Marmarosh et al., 2013).
Termination also presents the opportunity for members to consolidate the gains they have made in treatment. Here, the feedback process is useful as co-members and therapist can share their observations of the changes the departing member has made over treatment. This feedback should be combined with the member’s own self-perception of changes. Consolidation also includes coming to terms with what members have meant to one another. For example, in an open-ended group, the departing member might recall a memorable experience with each of the remaining group members.
This reflective process supports another therapeutic opportunity that termination presents—preparing for the future. The fear that some members experience upon leaving the group can be lessened by the recognition of the positive changes they have made. Still, members might be aware that challenges remain. In fact, in the feedback process, other members might identify areas of needed growth. For example, one member might say to another, “You’ve developed much more sensitivity to others’ feelings but sometimes when your anxiety is high, you don’t fully tune in.” The member having achieved an awareness of this growing edge can be assisted in developing a plan to address this area following termination (Bernard et al., 2008). Ideally, each member would leave with a roadmap for continuing their psychological work outside the group, a plan that is likely to bolster the member’s confidence in being able to manage without the support of the group. Anticipation of obstacles to continued progress, strategies for surmounting these obstacles, and awareness of strengths should be part of this plan (da Silva et al., 2021).
Therapist Strategies to Realize Termination Opportunities
Although the termination phase is rife with therapeutic opportunities, taking advantage of them requires particular therapist actions. For example, the therapist should aid a new member in an open-ended group in developing accurate expectations of the termination process. Primary topics to be pursued are how the determination will be made and how the process will unfold. The therapist might employ other members’ terminations as stimuli for non-terminating members to contemplate their eventual departures. Then, as termination approaches, the therapist should continually draw members’ attention to the interval between the current and last session (for example, in the case of a close-ended group, “Keep in mind we have only three sessions left.”), a reminder that “provides a sense of urgency and immediacy to the therapeutic process” (Mackenzie, 1996, p. 51).
Other interventions are directed toward particular goals of this stage, one of which is fostering members’ abilities to cope with the loss of the group. Assisting members in grappling with loss reactions requires cultivating the awareness that these reactions, whether accessible or not, are natural. The therapist’s action of inviting other members to respond when one member has identified a reaction promotes an experience of universality. The therapist, too, will have a range of feelings in relation to termination and can beneficially share them with members as a means of further conveying the notion that to grapple with loss is part and parcel of being human. Such disclosures also benefit the therapist for whom the need to mourn the ending also exists.
Processing loss reactions in a thorough way requires that members take stock of what they and the therapist mean to one another. Summative feedback is one way in which members unpack the significance of the group, and the therapist is likely to play a key role in facilitating feedback exchanges and other types of go-around to ensure that feedback is specific and balanced. Further, as members offer one another summative feedback, the therapist must ensure that feedback is not negatively biased based on members’ identity status. At the same time, the therapist should avoid imposing a level of structure that is so high that it blocks the free expression of feelings, some of which are likely to be shared by the therapist (Marmarosh et al., 2013).
Another way in which members honor their experiences in the group is through the creation and use of a ritual, a process by which the group establishes a metaphor that symbolizes the group and its work (Shapiro & Ginzberg, 2002). Rituals take highly varied forms, just as groups do, and can be created by the members collectively, the departing member, or the therapist. In the creation of the ritual, members unpack meanings of the group that might not have been previously evident. The ritual can then serve as a touchstone for members once they depart, reminding them of the lessons learned in the group and motivating them to apply the lessons. Culture often defines a person’s relationship with ritual, especially rituals concerning endings (Parkes et al., 2015). It is, therefore, helpful if the kinds of rituals groups employ are sufficiently flexible to accommodate members’ individual cultures. For example, in one group, a departing member presented each of the remaining members with a proverb, a piece of wisdom relevant to the recipient. This offering was congruent with the giver’s Native American culture in which the elders were seen as a source of wisdom to the community. By virtue of their readiness for departure, the member now saw themselves as passing to the status of group elder.
Another example of a ritual is one that comes from the group’s own unique experience as a group rather than members’ cultural backgrounds. In one group, members had employed the go-around as a means of ensuring that everyone had an opportunity to express their position on an issue facing the group. It was natural, then, that this group embraced a member’s suggestion of a go-around to encourage members to share their feelings about a departing member.
Special Circumstances
Most of the termination literature addresses the situation in which the member decides to leave the group, but at times, it is the therapist who ends a group, often due to some personal reason, such as illness, retirement, relocation, or the end of a segment of training (cf. Fieldsteel, 2005). This type of unilateral termination can lead members to see the therapist as putting personal needs ahead of the group members (Joyce et al., 2007b), a view likely to give rise to strong reactions of anger and mistrust. Members’ intense dependency longings stimulated by this change leads them to hope that in the remaining period, the therapist will fulfill all of members’ needs (Joyce et al., 1996). Although some therapists might develop a plan for a substitute therapist thereby creating the potential for some members to remain together, the group will essentially be a new group. The challenge for the therapist is to facilitate members in expressing all their reactions even though their doing so is likely to stimulate powerful negative reactions (for example, guilt) in the therapist. The therapist should also be vigilant and ready to address members’ efforts to protect the therapist from their pain.
Termination via suicide is one of the most challenging and painful occurrences any group psychotherapist must bear. It is especially difficult because the therapist must grapple with the devastation of the loss of the member, the sense of failure for not having prevented the suicide, worry about its effects on other members including suicide contagion and diminishment in their trust in the therapist, and fear of professional ramifications (e.g., litigation). Aside from the occasional article, the group psychotherapy community has largely neglected this topic, possibly conveying the message that it is too rare to address. However, the reality of group member suicide has been acknowledged, and the literature needs attention on this topic (e.g., O’Neill & Kueppenbender, 2012). Those who have addressed it have emphasized: (a) the usefulness of drawing on the trauma literature for guidance (Kibel, 1973); (b) the necessity of processing the event with the group members including the therapist’s openly sharing the members’ pain; and (c) the importance of consultation and supervision to address such challenging issues as whether the therapist and group members should attend the deceased member’s funeral.
Ethical Issues in Termination
Among the many ethical issues emerging at termination, three are highlighted here. First, therapists have a responsibility throughout a member’s participation in a psychotherapy group to monitor the member’s activity in the group to determine whether the member is ready for termination. This process is facilitated by routine outcome management (Kivlighan & Tasca, 2023; Muir et al., 2019) wherein the therapist obtains data about each member’s perceptions of benefits received over the course of the group. These data can be integrated with the therapist’s and other members’ observations. Were a member to demonstrate a failure to thrive in the group, the therapist would be obligated to consider whether termination and referral were in order or identify ways to better engage the member in the group. Second, when a member departs from the group, regardless of whether the termination is planned or unplanned, the therapist is obligated to take stock of the member’s continuing psychological needs and point to resources that the member can realistically access to meet them (Shapiro, 2010). For example, the therapist should strive to consider the member’s financial capabilities in identifying post-termination treatment opportunities. Third, the departing member(s) must be reminded that confidentiality continues even after the member’s tenure in the group is over, along with the cautionary statement that any violation of confidentiality could have serious ramifications for the member whose confidentiality is breached (Brabender & MacNair-Semands, 2022).
Summary
- There are different types of termination that may affect the group and its members’ experience of the process differently.
- Group members’ reactions to termination provide opportunities for exploration and growth.
- Individual group members’ identities and cultural background influence their experience of the termination process.
- Group members’ backgrounds and personal histories also influence how members might react to their own termination or that of other group members.
- Termination creates opportunities to review progress and discuss worries and hopes for the future beyond group therapy.
- Therapists can prepare group members for termination and facilitate the process by creating activities and rituals around it that resonate with the group.
Concurrent Therapies
This chapter presents an overview of recommended principles and practices when group psychotherapy is practiced concurrently with other treatments. These recommendations originate from review of the available clinical literature, composed primarily of extended case studies and expert opinion and supplemented by formal clinical research, although this is quite limited.
In essence, there are two primary structural arrangements of concurrent therapy: combined therapy and conjoint therapy. With respect to group psychotherapy, combined therapy refers to a patient receiving this modality along with another treatment, often either pharmacotherapy or individual therapy, with the same treater. When the treatments are well integrated, this arrangement allows for continuity and depth, as insights gathered in one modality can enrich and inform the other. In contrast, in conjoint therapy, a patient receives two treatment modalities, but with different therapists. For example, one clinician might conduct individual sessions while another leads a therapy group. This arrangement can offer diverse perspectives but requires careful coordination to avoid conflicting messages or misaligned therapeutic goals.
Another important designation regarding concurrent treatments is that they can be programmatic or emergent. In programmatic concurrent treatment, two or more treatments are bundled together from the start. When practiced conjointly, the treatments often occur in such settings as inpatient units or day treatment settings where the therapists have the opportunity to develop comprehensive and integrated formulations of the patient from more than one clinical perspective.
In emergent concurrent treatments, a client starts in one treatment, then a second treatment is added based on the clinical hypothesis that a more intensive and complex treatment approach may be advantageous for this particular patient. When practiced conjointly, the therapists may or may not be known to each other, and it is useful to find strategies, time, and effort to build a collaborative relationship. Individual and group outpatient psychodynamic psychotherapy is a paradigmatic example (Gans 1990).
Combined treatment tends to be more common in private practice, while conjoint treatment is more common in institutions and community mental health treatment centers (Yalom & Leszcz, 2020). In a similar fashion, emergent treatment is anecdotally more common in private practice, and programmatic treatment is more common in institutions and community mental health treatment centers.
The clinical and research literatures suggest that concurrent treatments that include a group component decreased drop-out rates and led to stronger outcomes (Arntz et al., 2022; Burlingame, et al., 2016; Linehan et al., 2015; Stone & Rutan, 1984; Yalom & Leszcz, 2020). Concurrent treatment may be particularly indicated where there is a higher level of clinical complexity or greater comorbidity in patient presentation, as in the treatment of those with both personality disorders and substance use disorders. This treatment modality may reflect an advantageous manner of engagement for clinicians treating those with the most severe difficulties in interpersonal functioning.
The advantages and challenges of concurrent treatments
The rationale for concurrent treatment lies in the hypothesis that different therapeutic modalities can interact synergistically, a dynamic Porter (1993) refers to as potentiation. He suggests that the two approaches may “magnify each other’s strengths,” with group therapy potentially enriching and amplifying the effects of individual treatment. This interplay could lead to a more effective therapeutic process and a shorter overall duration of care. Additionally, concurrent modalities may operate in a complementary fashion, with each addressing distinct and non-overlapping domains of psychological growth. Ormont (1981) captures this richness by describing these conjoint opportunities as encompassing multiple settings, transferences, observers, interpreters, and maturational agents. In particular, group therapy offers fertile ground for developing interpersonal awareness, while individual therapy supports deeper exploration of intrapsychic dynamics (cf. Kauff, 2009; Rutan & Alonso, 1982; Smolar, 2018, 2020; Ulman, 2002).
The work and the challenges
For the group therapist engaging in the practice of concurrent treatments, an essential aspect of the work is to explore the patient’s level and quality of engagement not only within the therapy group but in comparison with the other treatment modalities that the patient is participating in. Combined therapy allows for the therapist to observe the patient across more than one modality, which thus provides opportunities to develop more complex and comprehensive formulations than might be developed only from observations in the therapy group. Witnessing and exploring the patient’s differential responses across modalities could shed light on such dimensions as attachment styles, defensive needs, and sources of anxiety. These cross-modality observations also help determine whether the therapies are working in a complementary fashion—deepening, broadening, or reinforcing the therapeutic process—or whether antitherapeutic dynamics are emerging (Roth, 2009). Is there, for example, greater therapeutic alliance in individual therapy than in the group? To the extent there are differential levels of engagement across the modalities, the therapist needs to explore and generate hypotheses about the source of those differences. Is the patient, for example, splitting or polarizing the experiences in the two modalities, valuing the one-to-one intimacy of individual therapy and devaluing the more complex and potentially competitive world of the therapy group? How is the therapist reacting to these differential responses of the patient? Is the therapist colluding in this splitting, also finding greater value in one modality than in the other?
In conjoint therapy, the group therapist must not only track the patient’s differential relationships with each modality but also to each clinician. Is there greater therapeutic alliance, for example, with one clinician than with the other, and does this difference lead to different countertransference reactions in the treaters? Further, attention needs to be paid to the quality of the relationship between the treaters themselves. Is there mutual respect, and how well are the differences between them understood and contained? This complicated work requires an openness, humility, and collaborative spirit to sort out the nature and bases of these various differences, including differences in therapeutic style and approach, in assessment of patient progress, in valuing the treatment modalities, as well as in personal, professional and sociocultural identities. Providers should strive to attain a high degree of collaboration with one another whenever multiple treatments are being delivered. Separate modalities should not be prioritized over one another but should be understood as dialectical tools to further treatment objectives and patient goals. This is a dynamic tension, which requires openness to other providers’ views and understanding of how differences in perspectives come about. From an ethical perspective, it calls for a shared commitment to understanding how differences emerge and how they may be integrated to enhance therapeutic coherence and clinical effectiveness (Brabender & Fallon, 2009). Finally, concurrent treatments also require the treaters to be open and sensitive to questions about how sociocultural dynamics, values, and attitudes across patients, modalities, and treaters get played out and work to understand and contain them.
Concurrent treatment is often practiced when a patient engaged in group therapy is also receiving individual psychotherapy or working with a medication prescriber. These arrangements may be carried out in either a combined or conjoint fashion. In the case of medications, either psychotropic (cf. Fain et al., 2008; Mintz, 2022; Rodenhauser & Stone, 1993; Stone, et al., 1991) or psychedelic (Stauffer & Anderson, 2023; Trope et al., 2019), the work can be conducted either with a prescriber in one-to-one fashion or in a medication group setting.
Across all such scenarios, a central challenge for the group therapist is to integrate observations, hypotheses, and formulations arising within the group with clinical information from the other modality. Equally important is helping the patient link and synthesize therapeutic experiences across these modalities, ensuring that they do not remain disconnected or siloed from one another. In essence, the task for the group clinician is to maintain a boundary between the therapy group and the other modality that is neither too rigid nor too permeable. This boundary should allow for a meaningful linkage while preserving the integrity of each therapeutic enterprise (cf. Lipsius, 1991; Marmarosh, 2016). For example, if a patient abruptly announces in the therapy group the unilateral decision to stop medications, the group therapist could not only invite the patient to explore his thoughts and feelings about this in the group but, importantly, could explore with the prescriber their understandings about this and coordinate interventions that support the patient across both modalities (cf. Brabender & Fallon, 2009).
Concurrent treatments routinely occur in the context of intensive outpatient programs, inpatient psychiatric wards (Cook et al. 2014; Deering 2014; Snyder et al. 2012), and residential treatment facilities (Magliano et al., 2016) for substance abuse, psychiatric disorders, or both. In these settings, clients typically attend a variety of groups differing widely in formats, aims, processes and culture (SAMSHA, 2021;Wendt & Gone, 2017), such as 12-step self-help groups, skills training groups, and interpersonal or psychodynamic groups. For the sake of an integrated and coherent approach to treatment, it is incumbent upon the group therapist in one modality to be open to bridging differences with therapists steeped in very different models.
As discussed in the pre-group preparation chapter of the guidelines (Chapter 4), group members entering a program should be clearly informed about what to expect in the specific groups they will be attending. This orientation work allows them to fully consent (or not) to treatment with a clear understanding of what to expect and can thus facilitate their engagement with the work in each kind of modality.
Summary
- Patients may be in group therapy in conjunction with individual therapy, with 12-step groups, with pharmacotherapy, or in a setting with multiple other active treatments.
- There is some evidence suggesting decreased drop-out when using concurrent individual and group therapy.
- Combined concurrent treatment occurs when the same clinician delivers two treatments to the same patient, such as group and individual therapy or group and pharmacotherapy. Conjoint concurrent treatment occurs when different clinicians deliver the treatments.
- Concurrent treatment can emerge with one treatment added to another. It can also occur programmatically from the beginning of treatment.
- The essential work for the group therapist is to explore and make sense of the patient’s experiences not only in the group but across the varied clinical contexts, attending to differences and similarities in the patient’s needs, affective states, and motivations. This involves developing a comprehensive formulation that integrates the patient’s perspectives across treatment settings and, in the case of conjoint treatments, synthesizes the perspectives of the different treating clinicians.
Online Group Therapy Through Video
Although the use of group therapy through video started at the beginning of the 21st century, its main thrust occurred because of the sudden onset of the COVID-19 pandemic in 2020, as group therapists around the world had to quickly shift to online practice, often with minimal preparation or training (Weinberg, 2021; Zhang et al., 2025). A survey of group therapists by Gullo and colleagues (2022) reports that while therapists perceive the effectiveness of online groups to be determined by the same kinds of therapeutic processes (e.g., cohesion) and therapist qualities (e.g., presence) as in-person groups, they are less comfortable and satisfied with online work compared to face-to-face groups and find that the work of managing avoidance and conflict, fostering cohesion, and attending to nonverbal communication to be more difficult in online groups. In parallel studies, patients report that it is more difficult to connect to others in the group and to develop a sense of cohesion in the online groups compared to in person groups. Such preliminary studies underscore the importance of introducing guiding principles for the practice of online group therapy (Lopez et al., 2020, Sousa et al., 2025).
Models of online groups
In general, three models can be identified for online groups:
- Online only: All group members and the group therapist(s) are online all the meetings.
- Online with periodic in-person meetings: This model is highly recommended if possible.
- Hybrid: Some group members are online while others are in the same room with the group therapist. This model is not recommended, unless no other option is available. In that case, see below for applicable recommendations.
Benefits of online group therapy
Although the outcome literature on online groups is still limited, studies have shown that these types of groups can be as effective in creating positive change as groups meeting in-person (Khatri et al., 2014; Larsson et al., 2022; Park & Cha, 2023; Zhang et al., 2025). Specifically, some clients report experiencing the same levels of change in gaining insight and experiencing emotional change (Zhang et al., 2025.)
It has also been proposed that patients with avoidant/dismissive attachment style can benefit more from groups online than in person as the screen protects them from being overwhelmed, allowing them to be more expressive and attached in online groups (Weinberg, 2021). While there is value in recognizing that the online format may reduce a sense of intimacy for some clients, those with attachment difficulties may find it more helpful. The same phenomenon can occur with group members with social anxiety, as they may be less anxious online, which could help them be more engaged in the group. In fact, some research has shown that some clients find it easier to engage in deeper levels of group discussion and to express emotions in online groups than in in-person ones (Zhang et al., 2025).
Common barriers, pitfalls and challenges for online group therapy
Online groups pose specific challenges and obstacles compared to in-person groups. Most of them can be overcome or compensated for if group therapists use creative solutions:
The setting
When meeting in person, the setting is defined by the group therapist facilitating the creation of a safe holding environment or frame (see Chapter 1). The online group therapist has less control over the external boundary of the group; each group member decides about the space from which they connect, the chairs on which they sit, and the decoration of their background. This difference in where the members are physically located has the potential to pose greater risks in maintaining confidentiality and privacy in the home environment. Thus, the online group therapist should actively enlist the group members in the construction of a safe setting, a protective group container by informing them about the need to safeguard the therapy space at home.
The disembodied group
In addition to the decreased control over the physical space in online groups compared to in-person groups, another challenge unique to the practice of online therapy is the decreased availability of nonverbal cues, such as postural shifts and limb and hand movements that are a core aspect of interpersonal interactions as they communicate important affective states and needs (Weinberg, 2021; Yalom & Leszcz, 2020; Zhang et al., 2025). Compensating for this is the fact that facial expressions are clearer and larger on the screen than perceived in person. Group therapists can thus help the group become more sensitive to and curious about the meanings of facial expressions as they arise in the online group (Weinberg, 2024). For example, group therapists can encourage members to verbally express their reactions by modeling doing so and pointing out what they notice. While members don’t have access to others’ bodily cues, they can be encouraged to attend to their own non-verbal reactions and reflect upon and verbalize what they might signify about their own internal psychological states (Canales, 2024).
Relying on eye contact as another informative communicative channel in groups is lost in the online group; the screen doesn’t facilitate an understanding of who is looking at whom. The group therapist needs to help the group with this limitation by instructing group members to be explicit about who they are talking to.
Therapists providing services online should become more active than when meeting in their offices, asking the group members to move closer to or further from the camera (although the chosen distance may in itself reflect defensive needs), suggesting that they report their here-and-now somatic experiences (Yalom & Leszcz, 2020). Therapists can use the tone and pace of their voice to sooth a member when they are anxious. Various creative activities can be employed to increase the mindfulness and verbal expression of bodily held sensations and accelerate building of group cohesion, such as synchronized hand clapping hands, breathing exercises, or five-minute body warmup.
Creating group cohesion
Group members attending online groups may experience more difficulties creating a strong bond and cohesion. This has been observed by therapists (Gullo et al., 2022) and reported by some clients (Sousa et al., 2025; Zhang et al., 2025). Group facilitators should be mindful of this challenge and explore ways to increase a sense of cohesion in their groups. For instance, they can suggest that group members connect a few minutes before the meeting starts, mingle before the group, and create the liminal or transitional space that is missing online (see below). It might also be helpful to mention the very technical but extremely important issue of gallery versus speaker view and recommend that group members use the gallery view to enhance the group-as-a-whole experience. Group therapists could also utilize structured activities, such as icebreakers, mindfulness activities, or reporting on the week, at the beginning of their sessions to help group members feel connected before engaging with each other at a deeper level.
The question of presence
Presence refers to the full involvement of the group therapist, focusing on the needs and interests of the group members and not of the therapist (Geller, 2020); it is considered a core therapist factor that promotes positive outcome. Geller (2022) further defines therapeutic presence as being fully attuned to the clients (i.e., emotionally, physically, cognitively, and relationally). This process, according to Geller (2022), “optimizes the doing and technique of therapy” (p. 22). Through a strong therapeutic presence, clients feel seen and understood, which allows the formation of a strong working alliance (Andrews et al., 2024). The screen may challenge the group therapist to stay present (cf. Brahnam, 2014). Below are some ways to compensate and stay present (Frank, 2020; Geller, 2020; Guth et al., 2021; Weinberg, 2020a, 2020b, 2021).
- Using self-disclosure: The group therapist can increase the use of self-disclosure about their feelings regarding the here-and-now (e.g., “When you share your loss, I feel closer to you.”).
- Using imagination: The group therapist can make use of imagination and encourage group members to do the same. Imagining situations that occur in the in-person meeting (e.g., “Who would you like to sit next to you?”) can bring the group experience to the present.
- Being particularly open about therapeutic mistakes or failures (e.g., empathic failures) to be attuned to the group needs.
- Avoiding any type of multitasking while running an online group.
- Testing tools and platforms used for sessions before the beginning of the group meeting can help therapists stay present during the group without worry about technological issues if they arise.
- Coordinating with co-leaders to ensure that, if technological issues occur, one of the therapists present will stay engaged in the group process while the other will work on resolving the issue.
Videoconference fatigue
Döring and colleagues (2022) define videoconference fatigue as exhaustion (i.e., physical, emotional, and cognitive) caused by the use of videoconferencing systems. This concept might be particularly relevant for group members who, in addition to joining therapy groups online, also spend significant amounts of time in online meetings due to their employment or other circumstances. Group therapists should be mindful of the possibility that their group members may experience this phenomenon, or that they might also experience it themselves.
Group members’ videoconferencing fatigue can be addressed by monitoring the group’s and individual members’ level of energy in sessions (e.g., Does group members’ engagement and participation change throughout the sessions? Do group members appear distracted? Do group members seem to be multitasking?). Group leaders can include breaks during meetings to reduce telehealth fatigue (Amulya, 2020). They may also encourage the use of optimal technology (e.g., high-band connection, external microphone, wide angle camera, the use of a computer or laptop as opposed to a mobile phone) to maximize the clarity of audio and video signals to approximate the in-person experience. Guth et al., (2021) also recommends not exceeding two-hour long sessions and checking in regarding the group members’ physical needs (e.g., need to stand up and stretch, need to turn off one’s camera to ground) to help prevent videoconferencing fatigue.
Key considerations for online group therapy
Legal and ethical considerations
“Group psychotherapy is predicated on trust” (Brabender & MacNair-Semands, 2022, p. 26). While therapists can never fully guarantee that group members’ privacy and confidentiality won’t be breached by other members, some risks might be heightened in online groups (Yalom & Leszcz, 2020). More specifically, risks for loss of privacy and for breaches of confidentiality might be greater in online groups than in in-person groups. For instance, therapists cannot guarantee that no one external to the group (e.g., family member or roommate) will be overhearing the content of a session, that someone might walk in a members’ room during a session, or that clients’ internet connection is secure enough to prevent security breaches (Yalom & Leszcz, 2020). Group therapists should be very aware of these risks and never assume that the content of sessions is kept online the same way that it is kept in their offices. To minimize some of these risks on their end, therapists should always use secure internet connections and up-to-date software to minimize potential security breaches. On the clients’ end, the preparation session is particularly important to discuss these issues and help group members engage with the online group safely and securely. At the very least, therapists should emphasize the need to preserve group members’ confidentiality and privacy during the orientation of individual members and at times during the group sessions (see Chapters 1 and 4).
For United States-based therapists, two legal considerations should be checked before starting online groups: (1) whether the video platform or application used is HIPAA-compliant; and (2) licensing laws and regulations about practicing therapy across state lines. Group facilitators should ask where clients are located at the beginning of each session to ensure that they are in a state they are licensed or authorized to practice in.
The standard Informed consent should be adapted for the online setting. For example, therapists can add information about potential benefits and risks of video-conferencing (e.g., risks to patient confidentiality), the need for a back-up plan (e.g., phone number where they can be reached) to restart the session or to reschedule it in the event of technical problems, and the importance of informing the group leaders of their location in case of an emergency.
Preparing group members for online meetings
The standard practice of meeting group candidates individually before the group begins (see Chapter 4) also holds for online groups. When meeting with group members before the group starts (for screening, agreeing on the goals, and preparing for the group), group facilitators can help them understand the importance of keeping confidentiality, avoiding loss of privacy, and minimizing the distractions of the home environment. Informing group members about the importance of finding private spaces to attend sessions, using headphones (especially if not having access to a fully private space), avoiding email reading and texting, or having someone else attend to pets can be particularly helpful. Therapists can also address ways that clients can position themselves to optimize connection with other members, type of lighting to use, encouraging the use of headphone to help with privacy, etc.
The preparation meeting for online groups should also cover any technical items related to the platform that will be used to help clients be as prepared as possible to join the first session. This includes discussing how to access the platform, when and how access links will be shared, and what to do in case of loss of connection. Therapists may also consider demonstrating use of the platform to clients. The informed consent should be reviewed and therapists can help group members understand and minimize the potential risks discussed above. For instance, therapists should encourage participation with as little disruptions as possible in order to maximize engagement and protect other group member’s privacy. They can also discuss ways to protect the groups’ privacy and information (Yalom & Leszcz, 2020). Individual clients should understand that online services limit a therapists’ ability to respond to crises. Group leaders should make plans with clients about ways they may access emergency care if needed (Shore et al., 2018; Yalom & Leszcz, 2020). Finally, therapists should ensure that they have access to each group members’ phone number in order to be able to reach them in case of technical issues, sudden interruptions, or emergencies.
Diversity, identity, and cultural issues
The value of cultural humility, cultural opportunity, and cultural openness are no less important in online groups than in-person ones. When leading an online group, specific accessibility considerations should be taken by the group leaders. For instance, therapists should be aware of the impact of geographic and socioeconomic factors on technology access. Further, therapists should be able to assess and identify how a client’s cognitive, sensory, or motor function may impact their experience attending an online group, and implement appropriate accommodations (APA, 2024). Guth and colleagues (2021) recommend assessing the type of technology used by clients in addition to whether they have access to a stable and secure internet connection. Further, therapists should be trained in ways to use closed captioning or other forms of communication for group members with hearing loss, diverse information processing needs, or language skills (Guth et al., 2021). All accessibility considerations and adjustments should be discussed explicitly with group members during the preparation stage of the group, as well as in the initial sessions of a group.
Therapist Competence
Monitoring competence is one of the ethical imperatives of the group therapist (Brabender & MacNair-Semands, 2022). Just as being an effective individual therapist does not necessarily lead to becoming a skilled group therapist (see Chapter 1), it is not enough to be a competent in-person group therapist to succeed online. Leading groups online requires specialized training (APA, 2024; Yalom & Leszcz, 2020). This training should include topics mentioned in these guidelines, such as overcoming the obstacles of the absence of the body, knowing how to help the members create and maintain the holding environment, increasing the group cohesion in order to create a shared experience, ethical principles of telehealth provision, staying up-to-date on relevant laws and regulations, and understanding risks and benefits unique to telehealth.
Additional issues
Paying attention to the background
Shifting to online groups creates a window into the group members’ privacy, since most of them connect from home. Therapists should pay attention to their background and find ways to, when clinically relevant, insert their observations in the group discussion. It is easy to ignore events and movements occurring in the background, which therapists would never ignore in their offices (e.g., a stranger entering the room, a pet on the table whose tail appears on the camera). Being aware of these events is essential to creating a cohesive and safe group, especially as some of them might disrupt the sense of safety for all group members or have a dynamic meaning.
Therapists should also be mindful of their own background and decide what they want to disclose, analogous to considerations of how to decorate one’s office used in in-person work in terms of what it might reveal about the therapist’s person. Although having a private and confidential working space when working from home is highly recommended, using a virtual or blurred background could be helpful for therapists running groups from their home and not wanting to show anything personal. However, remember that it might bring more questions for the group members regarding what you try to hide. Curiosity about the backdrops, whether members’ or therapist’s, is to be expected.
Self-view—pros and cons
Seeing oneself on screen, just as looking in the mirror, while in the role of group member or therapist can evoke a variety of reactions, such as becoming increasingly anxious, self-absorbed, and self-conscious, and losing track of the group. Group members can turn off the camera, however, if they do it, they miss the opportunity of exploring important aspects of their self-image and reactions, and hiding self is likely to draw curiosity or concern from other group members and impact the group process. Boundaries around camera usage should be part of the group agreement and discussed with the group. On some platforms, clients may be able to turn off self-view without turning off their cameras. When applicable, this option should be discussed with group members.
Chat and outside group communication
The chat option can create a parallel channel of communication for group members. It can compete with the ongoing communication and might distract the group members’ attention and make it difficult for them to stay present. In addition, members might use it for private communication (addressing only specific group members privately), which breaches the common guidelines not to have secret outside interactions among members. This is a boundary issue that needs to be clarified as part of the group agreement, preparation, and ongoing maintenance of the boundary of the group. It is important to address this issue because members of the group may have online communication with one another either in the group or outside of the group. Some group therapists recommend disabling or limiting the use of the chat function while others note that its use might be helpful to have available in case of technical difficulties (Andrews et al., 2024).
Loss of liminal space
When the group meets online, the time and space before and after group therapy sessions are lost. These are transitional spaces where people have an opportunity to interact with one another, socialize, and be able to say a proper goodbye with the kinds of rituals that are routinely part of psychotherapy groups that meet person-to-person. Allied with the loss of the liminal space is a complaint that patients have about the loss of a boundary between their therapy world and their personal world and the need to create space moving from one to the other. A possible way to create this liminal space online is to invite people to join the application platform five to 10 minutes before the group meeting, thus creating an experience analogous to the waiting room. The group therapist can also allow the group to stay online five minutes after the meeting ends, analogous to informal congregating after the in-person session ends.
Using unique features that the technological platform provides
Some online platforms provide features that can improve the group function, enhancing the shared experience. For example, in groups using art therapy, the whiteboard or share screen function offered by some platforms can be used to create a shared art piece of the entire group. Some telehealth platforms allow the group therapist to move around the squares of the group members and to enforce this arrangement on all participants’ screens. This way, all group members share the same picture of groups seating. Therapists can choose a platform that best suits the type of services they provide and should ensure that the platform follows all laws and regulations related to the provision of mental health services (e.g., HIPAA compliance).
Co-leading online
As interactions online are limited, it is even more important for co-leaders to build a strong relationship with one another outside of the group, maximizing their sense of trust, synergy, and ability to check in with one another. This may need to be done more transparently in the group because of the lack of access to body language and nonverbal communication. Using the private chat function is not recommended, since it means communicating behind the back of the group members, and it might also mistakenly be sent to everyone. Co-leaders should learn to communicate with each other verbally in front of the group (Weinberg, 2020b). Co-leaders also need to connect with each other outside of the group session to discuss their experience, work on identifying ways to communicate with each other in the group, and debrief sessions.
The hybrid model (Zigenlaub & Stolper, 2024)
In this model, some of the group members are in the same room while others (sometimes one group member) are online. Although there is still no research about the effectiveness of this model, experience suggests that it can be problematic. It is difficult for members that are online to break the screen barrier, and they may need more attention from the group therapist, which creates dynamics of jealousy and competition. This model might suit groups that are already cohesive better than newer groups.
If a hybrid approach is necessary, the following suggestions have been found to be conducive in engaging online participants in a predominately in-person group (Weinberg, 2024):
- The display/computer representing remote participants should be positioned within the circle.
- The use of a wide-angle camera, a sensitive external microphone, and an external speaker greatly improves remote participants’ ability to follow the group.
- Hide self-view to maximize screen area.
- Leader(s) should periodically prompt remote participants to ensure engagement and connectivity.
- Co-leaders can actively lead even if they are participating remotely. In this case, the co-leader should have a separate computer and display, and their position within the circle should be as it would be located if they were physically in the room.
Summary
- An important, although as yet untested, hypothesis posits that online groups are as effective as in-person groups. Such research is needed to support the viability of online group work.
- Given the suggestion in the literature that cohesion is more difficult to foster in online groups, research is needed to compare and contrast the development of cohesion in these two settings. Further, the therapist working online should pay special attention to increase the shared experience.
- Given that participants are usually in their home environments, therapists should emphasize the need and challenges of maintaining privacy and confidentiality.
- The group therapist should find creative ways to overcome the obstacles inherent in the online modality, especially to overcome the lack of body-to-body communication and video fatigue.
- Members with avoidant/dismissive attachment style and social anxiety might benefit more from online group participation.
- When possible, it is recommended that the online group will meet also in-person from time to time.
References
Abernethy, A.D. (1998). Working with racial themes in group psychotherapy. Group, 22(1), 1-13. https://doi.org/10.1023/A:1023025500831
Abernethy, A.D. (2024). Addressing diversity dynamics in group therapy. Routledge. https://doi.org/10.4324/9781003455783
Abernethy, A.D. (2024). Addressing diversity dynamics in group therapy: Clinical and training applications. Routledge. https://doi.org/10.4324/9781003455783
Abernethy, A.D. (Ed.). (2024). Addressing diversity dynamics in group therapy. Routledge. https://doi.org/10.4324/9781003455783
Adi, A., & Mathbout, M. (2018). The duty to protect: Four decades after Tarasoff. American Journal of Psychiatry Residents’ Journal, 13(4), 6-8. https://doi.org/10.1176/appi.ajp-rj.2018.13040
Agazarian, Y. (1997). Systems-centered therapy for groups. Guilford Press.
Agazarian, Y. (2001). A systems-centered approach to inpatient group psychotherapy. Jessica Kingsley Publishers.
Alexander, F., & French, T. (1946). Psychoanalytic therapy: Principles and application. Ronald Press.
Alldredge, C.T., Burlingame, G.M., Yang, C., & Rosendahl, J. (2021). Alliance in group therapy: A meta-analysis. Group Dynamics: Theory, Research, and Practice, 25(1), 13-28. https://doi.org/10.1037/gdn0000135
American Association for Marriage and Family Therapy. (2015). Code of ethics. https://aamft.org/AAMFT/Legal_Ethics/Code_of_Ethics.aspx
American Counseling Association. (2014). ACA code of ethics. https://www.counseling,org/resource/ethics
American Group Psychotherapy Association. (2002). Recertification requirements. https://agpa.org/get-certified-cgp/recertification/
American Group Psychotherapy Association Diversity, Equity, and Inclusion Task Force (2023). Guidelines for creating affirming and restorative group experiences. https://agpa.org/guidelines-for-creating-affirming-and-restorative-group-experiences
American Psychological Association. (2017). Ethical principles of psychologists and code of conduct. https://www.apa.org/ethics/code/
American Psychological Association. (2017). Multicultural guidelines: An ecological approach to context, identity, and intersectionality. Retrieved from: http://www.apa.org/about/policy/multicultural-guidelines.pdf
American Psychological Association (2024). Guidelines for the practice of telepsychology. Retrieved from https://www.apa.org/about/policy/telepsychology-revisions.
Amulya, D.S.L. (2020). An experiment with online group counseling during COVID-19. In L.S.S. Manickam (Ed.), COVID-19 pandemic: Challenges and responses of psychologists from India (pp. 182-197). Centre for Applied Physiological Studies.
Andrews, K., Ross, D., & Maroney, T.L. (2024). Online group psychotherapy: A systematic review. Community Mental Health, 60, 1511-1531. https://doi.org/10.1007/s10597-024-01304-4
Arntz, A., Jacob, G.A., Lee, C.W., Brand-de Wilde, O.M., Fassbinder, E., Harper, R.P., Lavender, A., Lockwood, G., Malogiannis, I.A., Ruths, F.A., Schweiger, U., Shaw, I.A., Zarbock, G., & Farrell, J.M. (2022). Effectiveness of predominantly group schema therapy and combined individual and group schema therapy for borderline personality disorder: A randomized clinical trial. JAMA Psychiatry, 79(4), 287-299. Doi: 10.1001/jamapsychiatry.2022.0010
Aron, C.M., & Lefay, S.M. (2024). Hidden diversity: The invisible oppressor of classism. In. A.A. Abernathy (Ed.), Addressing diversity dynamics in group therapy: Clinical and training application (pp. 65-78). Routledge. https://doi.org/10.4324/9781003455783
Baker, E., Burlingame, G.M., Cox, J.C., Beecher, M.E., & Gleave, R.L. (2013). The Group Readiness Questionnaire: A convergent validity analysis. Group Dynamics: Theory, Research, and Practice, 17(4), 299–314. https://doi.org/10.1037/a0034477
Bales, R.F. (1950). Interaction process analysis: A method for the study of small groups. Addison-Wesley.
Barlow, S.H. (2012). An application of the competency model to group-specialty practice. Professional Psychology, 43(5), 442-451. http://dx.doi.org/10.1037/a0029090
Barlow, S.H. (2013). Specialty competencies in group psychology. Oxford University Press. https://doi.org/10.1093/med:psych/9780195388558.001.0001
Beck, A., & Lewis, C.S. (Eds.). (2000). The process of group psychotherapy: Systems for analyzing change. American Psychological Association. https://doi.org/10.1037/10378-000
Belcher Platt, A.A. (2017). Racial-cultural events and microaggressions in group counseling as perceived by group counseling members of color. ETD Collection for Fordham University. AAI10607840. Retrieved from https://research.library.fordham.edu/dissertations/AAI10607840
Bemak, F., & Chung, R.C.-Y. (2019). Race dialogues in group psychotherapy: Key issues in training and practice. International Journal of Group Psychotherapy, 69(2), 172-191. https://doi.org/10.1080/00207284.2018.1498743
Bernard, H., Burlingame, G., Flores, P., Greene, L., Joyce, A., Kobos, J.C., Leszcz, M., MacNair-Semands, R.R., Piper, W.E., Slocum McEneaney, A.M., & Feirman, D. (2008). Clinical practice guidelines for group psychotherapy. International Journal of Group Psychotherapy, 58(4), 455-542. https://doi.org/10.1521/ijgp.2008.58.4.455
Bieling, P., McCabe, R.E., & Antony, M. (2022). Cognitive behavioral therapy in groups (2nd ed.). Guilford.
Bion, W.R. (1961). Experiences in groups. Basic Books.
Bion, W.R. (1962). Learning from experiences in groups. Basic Books.
Bogdanoff, M., & Elbaum, P. (1978). Role lock: Dealing with monopolizers, mistrusters, isolates, helpful Hannahs, and other assorted characters in group psychotherapy. International Journal of Group Psychotherapy, 28(2), 247-262. https://doi.org/10.1080/00207284.1978.11491610
Bohm, D. (2010). On dialogue. Routledge Classics.
Brabender, V. (2010). Group development. In R.K. Conyne (Ed.), The Oxford handbook of group counseling (pp.182-204). Oxford University Press.
Brabender, V., & Fallon, A. (2009). Group development in practice: Guidance for clinicians and researchers on stages and dynamics of change. American Psychological Association. https://doi.org/10.1037/11858-000
Brabender, V., & Fallon, A. (2019). Group psychotherapy in inpatient, partial hospital, and residential care. American Psychological Association.
Brabender, V.M., & Fallon, A. (2009). Ethical hot spots of combined individual and group therapy: Applying four ethical systems. International Journal of Group Psychotherapy, 59(1), 127–147. https://doi.org/10.1521/ijgp.2009.59.1.127
Brabender, V., & MacNair-Semands, R. (Eds.) (2022). The ethics of group psychotherapy: Principles and practical strategies. Routledge. https://doi.org/10.4324/9781003105527
Brabender, V., & MacNair-Semands, R. (2022). The ethics of group psychotherapy: Principles and practical strategies (1st ed.). Routledge. https://doi.org/10.4324/9781003105527
Brahnam, S. (2014). Therapeutic presence in mediated psychotherapy: The uncanny stranger in the room. In G. Riva, J. Waterworth, & D.M. Murray (Eds.), Interacting with presence: HCI and the sense of presence in computer-mediated environments (pp. 123–138). Walter De Gruyter.
Brown, N. (2010). Group leadership teaching and training: Methods and issues. In R.K. Conyne (Ed.), The Oxford handbook of group counseling (pp. 346-369). Oxford Press. https://doi.org/10.1521/ijgp.2014.64.1.123
Brown, N. (2023). Teaching facilitation of group therapy: Processes and applications. Routledge. https://doi.org/10.4324/9781003329787
Burlingame, G., Fuhriman, A., & Johnson, J. (2002). Cohesion in group psychotherapy. In, J. Norcross (Ed.), Psychotherapy relationships that work: Therapist contributions and responsiveness to patients (pp. 71-87). Oxford University Press.
Burlingame, G.M., Cox, J.C., Davies, D.R., Layne, C.M., & Gleave, R. (2011). The Group Selection Questionnaire: Further refinements in group member selection. Group Dynamics: Theory, Research, and Practice, 15(1), 60–74. https://doi.org/10.1037/a0020220
Burlingame, G.M., & Jensen, J.L. (2017). Small group process and outcome research highlights: A 25-year perspective. International Journal of Group Psychotherapy, 67(1), S194-S218. https://doi.org/10.1080/00207284.2016.1218287
Burlingame, G.M., MacKenzie, K.R., & Strauss, B. (2006). Small-group treatment: Evidence for effectiveness and mechanisms of change. In J.C. Norcross, L.E. Beutler, & R.F. Levant (Eds.), Evidence-based practices in mental health: Debate and dialogue on the fundamental questions (pp. 309–320). American Psychological Association. https://doi.org/10.1037/11265-000
Burlingame, G.M., McClendon, T., & Yang, C. (2018). Cohesion in group therapy: A meta-analysis. Psychotherapy, 55(4), 384–398. https://doi.org/10.1037/pst0000173
Burlingame, G.M., Seebeck, J.D., Janis, R.A., Whitcomb, K.E., Barkowski, S., Rosendahl, J., & Strauss, B. (2016). Outcome differences between individual and group formats when equivalent and nonequivalent treatments, patients, and doses are compared: A 25-year meta-analytic perspective. Psychotherapy: Theory, Research and Practice, 53(4), 446-461. https://doi.org/10.1037/pst0000090
Burlingame, G.M., Strauss, B., & Joyce, A.J. (2013). Change mechanisms and effectiveness of small group treatments. In M.J. Lambert (Ed.), Bergin and Garfield’s handbook of psychotherapy and behaviour change (6th ed., pp. 640-689). John Wiley & Sons, Inc.
Burnes, T.R. (2020). Two stars and a wish: Termination activities for groups with sexual- and gender-identity diverse clients. In Homework assignments and handouts for LGBTQ+ clients (pp. 212-216). Routledge. https://doi.org/10.4324/9781003088639
Burnes, T.R., & Ross, K.L. (2010). Applying social justice to oppression and marginalization in group process: Interventions and strategies for group counselors. The Journal for Specialists in Group Work, 35(2), 169-176. https://doi.org/10.1080/01933921003706014
Canales, C. (2024). Somatic experiencing informed group psychotherapy online. In H. Weinberg, A. Rolnick, & A. Leighton (Eds.), The virtual group therapy circle: Advances in online group theory and practice (pp. 233-245). Routledge. https://doi.org/10.4324/9781003248606
Canuto, A., Meiler‐Mititelu, C., Herrmann, F., Giannakopoulos, P., & Weber, K. (2008). Impact of personality on termination of short‐term group psychotherapy in depressed elderly outpatients. International Journal of Geriatric Psychiatry, 23(1), 22-26. https://doi.org/10.1002/gps.1829
Castonguay, L.G., Barkham, M., Youn, S.J., & Page, A.C. (2021). Practice-based evidence—Findings from routine clinical settings. In M. Barkham, W. Lutz, & L.G. Castonguay (Eds.), Bergin and Garfield’s handbook of psychotherapy and behavior change: 50th anniversary edition (7th ed., pp. 191–222). John Wiley & Sons, Inc.
Chang, C.R., Ciliberti, A.A., & Kaklauskas, F.J. (2017). Mindfulness approaches to groups in college counseling centers. In J.M. Gross, M.D. Ribeiro, & M. Turner (Eds.), The college counselor’s guide to group psychotherapy (pp. 218-238). Routledge.
Chang-Caffaro, S., & Caffaro, J. (2021). When coleaders differ: Rupture and repair in group psychotherapy. American Journal of Psychotherapy, 74(2), 76-82. https://doi.org/10.1176/appi.psychotherapy.20200035
Chen, E.C., Thombs, B.D., & Costa, C.I. (2003). Building connection through diversity in group counseling. In D.B. Pope-Davis, H.L.K. Coleman, W.M. Liu, & R.L. Toporek (Eds.), Handbook of multicultural competencies in counseling and psychology (pp. 456-477). Sage Publications, Inc.
Chen, E.C., Kakkad, D., & Balzano, J. (2008). Multicultural competence and evidence-based practice in group therapy. Journal of Clinical Psychology, 64(11), 1261-1278. https://doi.org/10.1002/jclp.20533
Comas-Díaz, L., & Rivera, E.T. (Eds.). (2020). Liberation psychology: Theory, method, practice, and social justice. American Psychological Association. https://doi.org/10.1037/0000198-000
Comas-Díaz, L., Hall, G.N., & Neville, H.A. (2019). Racial trauma: Theory, research, and healing: Introduction to the special issue. American Psychologist, 74(1), 1–5. https://doi.org/10.1037/amp0000442
Cone-Uemura, K., & Bentley, E.S. (2017). Multicultural/diversity issues in group. In M.D. Ribeiro, J.M. Gross, & M.M. Turner (Eds.), The college counselor’s guide to group psychotherapy (pp. 21-35). Routledge. https://doi.org/10.4324/9781315545455
Cook, W.G., Arechiga, A., Dobson, L.A., & Boyd, K. (2014). Brief heterogeneous inpatient psychotherapy groups: A process-oriented psychoeducational (POP) model. International Journal of Group Psychotherapy, 64(2), 180-206. https://doi.org/10.1521/ijgp.2014.64.2.180
Cornish, M.A., Wade, N.G., Tucker, J.R., & Post, B.C. (2014). When religion enters the counseling group: Multiculturalism, group processes, and social justice. The Counseling Psychologist, 42(5), 578-600. https://doi.org/10.1177/0011000014527001
Counselman, E. (2005). Containing and using powerful therapist reactions. In L. Motherwell & J. Shay (Eds.), Complex dilemmas in group therapy: Pathways to resolution (pp. 155-165). Routledge. https://doi.org/10.4324/9780203021071
Crits-Christoph, P., Gibbons, M.B.C., & Mukherjee, D. (2013). Psychotherapy process-outcome research. In M.J. Lambert (Ed.), Bergin and Garfield’s handbook of psychotherapy and behavior change (6th ed., pp. 298–340). Wiley.
Dalal, F. (2002). Race, colour and the process of racialization: New perspectives from group analysis, psychoanalysis, and sociology. Brunner-Routledge.
Dalal, F. (2016). The individual and the group: The twin tyrannies of internalism and individualism. Transactional Analysis Journal, 46(2), 88–100.
da Silva, A.N., Ferreira, J.F., Conceição, N., Vaz Velho, C., & Vasco, A.B. (2021). Termination in psychotherapy: Contributions of an integrative metamodel. Journal of Psychotherapy Integration. https://doi.org/10.1037/int0000235
Deering, C.G. (2014). Process-oriented inpatient groups: Alive and well? International Journal of Group Psychotherapy, 64(2), 164-179. https://doi.org/10.1521/ijgp.2014.64.2.164
Döring, N., Moor, K.D., Fiedler, M., Schoenenberg, K., & Raake, A. (2022). Videoconference fatigue: A conceptual analysis. International Journal of Environmental Research and Public Health, 19(4), 2061. https://doi.org/10.3390/ijerph19042061
Eason, E.A. (2009). Diversity and group theory, and research. International Journal of Group Psychotherapy, 59(4), 563-574. https://doi.org/10.1521/ijgp.2009.59.4.563
Elias, N. (1994). Introduction. In N. Elias and J.L. Scotson (Eds.), The established and the outsiders (pp. xv–lii). Sage. (Original work published 1976)
Fain, D.S., Sharon, A., Moscovici, L., & Schreiber, S. (2008). Psychotropic medication from an object relations theory perspective: an analysis of vignettes from group psychotherapy. International Journal of Group Psychotherapy, 58(3), 303–326. https://doi.org/10.1521/ijgp.2008.58.3.303
Farhoudi, F., Artounian, V., & Michel, L. (2023). Culture, gender, and aggression in psychodynamic group therapy: A case of a male-only group with female leaders in Iran. International Journal of Group Psychotherapy, 73(4), 289-311. https://doi.org/10.1080/00207284.2023.2288857
Fei, W., Josselson, R., & Leszcz, M. (2023). When Chinese culture encounters western interpersonal group psychotherapy. International Journal of Group Psychotherapy, 73(4), 261-288. https://doi.org/10.1080/00207284.2023.2276488
Ferguri, L. (2001). The technique of group treatment: The collected papers of Louis R. Ormont, Ph.D. Psychosocial Press.
Fieldsteel, N.D. (1990). The termination phase of combined therapy. Group, 14(1), 27–32. https://doi.org/10.1007/BF01458121
Fieldsteel, N.D. (2005). When the therapist says goodbye. International Journal of Group Psychotherapy, 55(2), 245–279. https://doi.org/10.1521/ijgp.55.2.245.62191
Frank, R. (2020). Developing presence online. The Humanistic Psychologist, 48(4), 369-372. https://doi.org/10.1037/hum0000208
Frey, L.R. (2000). Diversifying our understanding of diversity and communication in groups: Dialoguing with Clark, Anand, and Roberson (2000). Group Dynamics: Theory, Research and Practice, 4(3), 222-229. https://doi.org/10.1037/1089-2699.4.3.222
Gans, J. (1990). Broaching and exploring the question of combined group and individual therapy. International Journal of Group Psychotherapy, 40, 123-137. https://doi.org/10.1080/00207284.1990.11490595
Garceau, C., Chyurlia, L., Baldwin, D., Boritz, T., Hewitt, P.L., Kealy, D., Söchting, I., Mikail, S.F., & Tasca, G.A. (2021). Applying the rupture resolution rating system (3RS) to group therapy: An evidence-based case study. Group Dynamics: Theory, Research, and Practice, 25(1), 89–105. https://doi.org/10.1037/gdn0000137
Gelso, C.J., & Kline, K.V. (2022). Some directions for research and theory on countertransference. Psychotherapy Research, 32(1), 59-64. https://doi.org/10.1080/10503307.2021.1968529
Geller, S. (2020). Cultivating online therapeutic presence: strengthening therapeutic relationships in teletherapy sessions. Counselling Psychology Quarterly, 34(3-4), 687-703. https://doi.org/10.1080/09515070.2020.1787348
Geller, S. (2022). Being present and together while apart: Therapeutic presence in telepsychotherapy. In H. Weinberg, A. Rolnick, & A. Leighton (Eds.), Advances in online therapy (pp. 21-34). Routledge. https://doi.org/10.4324/9781003205029
Gibbard, G.S., Hartman, J.J., & Mann, R.D. (1974). Group process and development. In G.S. Gibbard, J.J. Hartman, & R.D. Mann (Eds.), Analysis of groups (pp. 83-93). Jossey-Bass.
Gibbard, G.S., Hartman, J., & Mann, R.D. (1974). The individual and the group. In G.S. Gibbard, J. Hartman, & R.D. Mann (Eds.), Analysis of groups (pp. 177-196). Jossey-Bass.
Goodman, R.D., Williams, J.M., Chung, R.C.Y., Talleyrand, R.M., Douglass, A.M., McMahon, H.G., & Bemak, F. (2015). Decolonizing traditional pedagogies and practices in counseling and psychology education: A move towards social justice and action. In R.D. Goodman & P.C. Gorski (Eds.), Decolonizing “multicultural” counseling through social justice (pp. 147-164). Springer Science + Business Media. https://doi.org/10.1007/978-1-4939-1283-4
Greene, L.R. (1983). On fusion and individuation processes in small groups. International Journal of Group Psychotherapy, 33(1), 3-19. https://doi.org/10.1080/00207284.1983.11491741
Greene, L.R. (1999). Representations of the group-as-a-whole: Personality, situational and dynamic determinants. Psychoanalytic Psychology, 16(3), 403-425. https://doi.org/10.1037/0736-9735.16.3.403
Greene, L.R. (2024). CBT meets process: Assimilative integration with reference to group psychotherapy. International Journal of Group Psychotherapy, 74(1), 1–32. https://doi.org/10.1080/00207284.2024.2323613
Greene, L.R., Barlow, S., & Kaklauskas, F.J. (2020). Therapeutic factors. In F.J. Kaklauskas & L.R. Greene (Eds.), Core principles of group psychotherapy: An integrated theory, research, and practice training manual (pp. 54-70). Routledge. https://doi.org/10.4324/9780429260803
Greene, L.R., & Kaklauskas, F.J. (2020). Anti-therapeutic, defensive, regressive, and challenging group processes and dynamics. In F.J. Kaklauskas & L.R. Greene (Eds.), Core principles of group psychotherapy: An integrated theory, research, and practice training manual (pp. 71-85). Routledge. https://doi.org/10.4324/9780429260803
Greene, L.R., Kaklauskas, F.J., & Rutan, J.S. (2020). Advanced skills. In F.J. Kaklauskas & L.R. Greene (Eds.), Core principles of group psychotherapy: An integrated theory, research, and practice training manual (1st ed., pp. 121-139). Routledge. https://doi.org/10.4324/9780429260803
Griner, D., Erekson, D.M., Beecher, M.E., Cattani, K., & Burlingame, G.M. (2022). The power of compassion in group psychotherapy. Journal of Clinical Psychology, 1-12. https://doi.org/10.1002/jclp.23358
Gullo, S., Lo Coco, G., Leszcz, M., Marmarosh, C.L., Miles, J.R., Shechtman, Z., Weber, R., & Tasca, G.A. (2022). Therapists’ perceptions of online group therapeutic relationships during the COVID-19 pandemic: A survey-based study. Group Dynamics: Theory, Research, and Practice, 26(2), 103–118. https://doi.org/10.1037/gdn0000189
Guth, L.J., Pepper, E.L., Stephens, A.F., Pollard-Kosidowski, B.L., & Garrow, J. (2021). Ten tips for the facilitation of virtual groups. The Journal for Specialists in Group Work, 46(4), 309-321. https://doi.org/10.1080/01933922.2021.1984620
Haen, C., & Webb, N.B. (Eds.). (2019). Creative arts-based group therapy with adolescents: Theory and practice. Routledge. https://doi.org/10.4324/9780203702000
Hardy, K.V., & Bobes, T. (2016). Culturally sensitive supervision and training: Diverse perspectives and practical applications. Routledge. https://doi.org/10.4324/9781315648064
Hartman, J., & Gibbard, G.S. (1974). A note on fantasy themes in the evolution of group culture. In G.S. Gibbard, J. Hartman, & R.D. Mann (Eds.), Analysis of groups (pp. 315-336). Jossey-Bass.
Hays, P.A. (2016). Addressing cultural complexities in practice: Assessment, diagnosis, and therapy (3rd ed.). American Psychological Association. https://doi.org/10.1037/14801-000
Hewitt, P.L., Mikail, S.F., Flett, G.L., & Dang, S.S. (2018). Specific formulation feedback in dynamic-relational group psychotherapy of perfectionism. Psychotherapy, 55(2), 179-185. https://doi.org/10.1037/pst0000137
Holmes, J.G. (2002). Interpersonal expectations as the building blocks of social cognition: An interdependence theory perspective. Personal Relationships, 9(1), 1-26. https://doi.org/10.1111/1475-6811.00001
Hopper, E. (2003). Incohesion: Aggregation/massification. In R.M. Lipgar & M. Pines (Eds.), Building on Bion: Roots. Jessica Kingsley.
Hopson, R. (2024). The work of overcoming racism/white supremacy in group. In A.A. Abernathy (Ed.), Addressing diversity dynamics in group therapy: Clinical and training applications (pp. 136-151). Routledge.
Horvath, A.O. (2001). The alliance. Psychotherapy: Theory, Research, Practice, Training, 38(4), 365-372. https://doi.org/10.1037/0033-3204.38.4.365
Horvath, A.O., & Greenberg, L.S. (1989). Development and validation of the Working Alliance Inventory. Journal of Counseling Psychology, 36(2), 223-233. https://doi.org/10.1037/0022-0167.36.2.223
Horwitz, L. (1983). Projective identification in dyads and groups. International Journal of Group Psychotherapy, 33(3), 259-279.
Jimenez, D.E., Park, M., Rosen, D., Joo, J.H., Garza, D.M., Weinstein, E.R., Conner, K., Silva, C., & Okereke, O. (2022). Centering culture in mental health: Differences in diagnosis, treatment, and access to care among older people of color. American Journal of Geriatric Psychiatry, 30(11), 1234-1251. https://doi.org/10.1016/j.jagp.2022.07.001
Janis, I.L. (1972). Victims of groupthink. Houghton Mifflin.
Johnson, J.M., & Lambie, G.W. (2013). Ethnic identity and social‐cognitive maturity in a multicultural group experience. Counselor Education and Supervision, 52(3), 193-206. https://doi.org/10.1002/j.1556-6978.2013.00037.x
Joyce, A.S., Duncan, S.C., Duncan, A., Kipnes, D., & Piper, W.E. (1996). Limiting time-unlimited group psychotherapy. International Journal of Group Psychotherapy, 46(1), 61-79. https://doi.org/10.1080/00207284.1996.11491484
Joyce, A.S., & Marmarosh, C.L. (2023). Group selection, group composition, and pre-group preparation. In R. MacNair-Semands & M. Whittingham (Eds.), Group psychotherapy assessment and practice: A measurement-based care approach (pp. 31-82). Routledge. https://doi.org/10.4324/9781003255482-2
Joyce, A.S., McCallum, M., Piper, W.E., & Ogrodniczuk, J.S. (2000). Role behavior expectancies and alliance change in short-term individual psychotherapy. Journal of Psychotherapy Practice & Research, 9(4), 213–225.
Joyce, A.S., Piper, W.E., Ogrodniczuk, J.S., & Klein, R.H. (2007a). Patient characteristics and variations in termination processes and outcomes. In A.S. Joyce, W.E. Piper, J.S. Ogrodniczuk, & R.H. Klein (Eds.), Termination in psychotherapy: A psychodynamic model of processes and outcomes (pp. 109–131). American Psychological Association. https://doi.org/10.1037/11545-006
Joyce, A.S., Piper, W.E., Ogrodniczuk, J.S., & Klein, R.H. (2007b). Therapist-initiated termination. In A.S. Joyce, W.E. Piper, J.S. Ogrodniczuk, & R.H. Klein (Eds.), Termination in psychotherapy: A psychodynamic model of processes and outcomes (pp. 157–165). American Psychological Association. https://doi.org/10.1037/11545-008
Kaklauskas, F.J. (2021). Microaggression and group psychotherapy. The Group Circle (Spring 2021). American Group Psychotherapy Association.
Kaklauskas, F.J., & Greene, L.R. (Eds.). (2020). Core principles of group psychotherapy: An integrated theory, research, and practice training manual. Routledge. https://doi.org/10.4324/9780429260803
Kaklauskas, F.J., & Nettles, R. (2020). Towards multicultural and diversity proficiency as a group psychotherapist. In F.J. Kaklauskas & L.R. Greene (Eds.), Core principles of group psychotherapy: An integrated theory, research, and practice training manual (pp. 25-45). Routledge. https://doi.org/10.4324/9780429260803
Kaklauskas, F.J., & Olson, E.A. (2020). History and contemporary developments. In F.J. Kaklauskas & L.R. Greene (Eds.), Core principles of group psychotherapy: An integrated theory, research, and practice training manual (pp. 3-24). Routledge. https://doi.org/10.4324/9780429260803
Kaplan, S.A. (2017). The art of the sell: Marketing groups. In M.D. Ribeiro, J. Gross, & M.M. Turner (Eds.), The college counselor’s guide to group psychotherapy (pp. 117-130). Routledge. https://doi.org/10.4324/9781315545455
Kauff, P.F. (2009). Transference in combined individual and group psychotherapy. International Journal of Group Psychotherapy, 59(1), 29–46. https://doi.org/10.1521/ijgp.2009.59.1.29
Kealy, D., Ogrodniczuk, J.S., Piper, W.E., & Sierra-Hernandez, C.A. (2016). When it is not a good fit: Clinical errors in patient selection and group composition in group psychotherapy. Psychotherapy, 53(3), 308-313. https://doi.org/10.1037/pst0000069
Kernberg, O.F. (1980). Regression in groups: Some clinical findings and theoretical implications. Journal of Personality & Social Systems, 2, 51-75.
Khatri, N., Marziali, E., Tchernikov, I., & Sheppard, N. (2014). Comparing telehealth-based and clinic-based group cognitive behavioral therapy for adults with depression and anxiety: A pilot study. Clinical Interventions, 9, 765-770. https://doi.org/10.2147/CIA.S57832
Kibel, H.D. (1973). A group member’s suicide: Treating collective trauma. International Journal of Group Psychotherapy, 23(1), 42-53. https://doi.org/10.1080/00207284.1973.11492208
Kibel, H.D. (1981). A conceptual mode for short-term inpatient group psychotherapy. American Journal of Psychiatry, 138(1), 74-80. https://doi.org/10.1176/ajp.138.1.74
Kinouani, G. (2020). Silencing, power and racial trauma in groups. Group Analysis, 53(2), 145-161. https://doi.org/10.1177/0533316420908974
Kivlighan, D.M., Jr., & Holmes, S.E. (2004). The importance of therapeutic factors: A typology of therapeutic factors studies. In J.L. DeLucia-Waack, D.A. Gerrity, C.R. Kalodner & M.T. Riva (Eds.), Handbook of group counseling and psychotherapy (pp. 23-36). Sage Publications Ltd. https://doi.org/10.4135/9781452229683.n2
Kivlighan, D.M., Jr., London, K., & Miles, J.R. (2012). Are two heads better than one? The relationship between number of group leaders and group members, and group climate and group member benefit from therapy. Group Dynamics: Theory, Research, and Practice, 16(1), 1-13. https://doi.org/10.1037/a0026242
Kivlighan, D.M. III, & Chapman, N.A. (2018). Extending the multicultural orientation (MCO) framework to group psychotherapy: A clinical illustration. Psychotherapy, 55(1), 39-44. https://doi.org/10.1037/pst0000142
Kivlighan, D.M. III., Swancy, A.G., Smith, E., Brennaman, C. (2021). Examining racial microaggressions in group therapy and the buffering role of members’ perceptions of their group’s multicultural orientation. Journal of Counseling Psychology, 68(5), 621-628. https://doi.org/10.1037/cou0000531
Klein, R.H. (1996). Introduction to special section on termination and group therapy. International Journal of Group Psychotherapy, 46(1), 1-4. https://doi.org/10.1080/00207284.1996.11491480
Klein, R.H. (2008). Toward the establishment of evidence-based practices in group psychotherapy. International Journal of Group Psychotherapy, 58(4), 441-454. https://doi.org/10.1521/ijgp.2008.58.4.441
Leszcz, M. (2014). Reflections on the abuse of power, control, and status in group psychotherapy and group organizations. International Journal of Group Psychotherapy, 64(1), 124-130. https://doi.org/10.1521/ijgp.2014.64.1.124
Li, X., Kivlighan, D.M., Jr., Paquin, J.D., & Gold, P.B. (2021). What was that session like? An empirically-derived typology of group therapy sessions. Group Dynamics: Theory, Research, and Practice, 25(2), 107–121. https://doi.org/10.1037/gdn0000139
Lipgar, R.M., & Pines, M. (Eds.). (2003). Building on Bion: Roots. Jessica Kingsley Publishers.
Lo Coco, G., Tasca, G.A., Hewitt, P.L., Mikail, S.F., & Kivlighan, D.M., Jr. (2019). Ruptures and repairs of group therapy alliance: An untold story in psychotherapy research. Research in Psychotherapy, 22(1). https://doi.org/10.4081/ripppo.2019.352
Loshak, R. (1992). Combined group and individual therapy: A review of the literature. International Journal of Group Psychotherapy, 42(1), 3-19. https://doi.org/10.1080/00207284.1992.11490756
Lott, B. (2002). Cognitive and behavioral distancing from the poor. American Psychologist, 57(2), 100-110. https://doi.org/10.1037/0003-066X.57.2.100
Luca, M., & Lantieri, L. (2021). Termination as a developmental achievement in group psychotherapy. International Journal of Group Psychotherapy, 71(2), 201-218. https://doi.org/10.1080/00207284.2020.1865794
Lui, P.P., & Quezada, L. (2019). Associations between microaggression and adjustment outcomes: A meta-analytic and narrative review. Psychological Bulletin, 145(1), 45-78. https://doi.org/10.1037/bul0000172
Magee, R.V. (2019). The inner work of racial justice: Healing ourselves and transforming our communities through mindfulness. Tarcher Perigee.
Mahon, L., & Leszcz, M. (2017). The interpersonal model of group psychotherapy. International Journal of Group Psychotherapy, 67(1). http://dx.doi.org/10.1080/00207284.2016.1218286
Marmarosh, C., & Magenheimer, M. (2018). Applications of attachment research: Evidence you can apply to your group. International Journal of Group Psychotherapy, 68(3), 459–464. https://doi.org/10.1080/00207284.2018.1456801
Marziali, E., Munroe-Blum, H., & McCleary, L. (1997). The effects of combined individual and group psychotherapy on the treatment of borderline personality disorder. American Journal of Psychiatry, 154(10), 1460-1466. https://doi.org/10.1176/ajp.154.10.1460
MacKenzie, K.R. (1997). Clinical application of group development ideas. Group Dynamics: Theory, Research, and Practice, 1(4), 275–287. https://doi.org/10.1037/1089-2699.1.4.275
MacKenzie, K.R., & Livesley, W.J. (1983). A developmental model for brief group therapy. In R.R. Dies & K.R. MacKenzie (Eds.), Advances in group psychotherapy: Integrating theory and research (pp. 101–135). International Universities Press.
MacNair, R.R., & Corazzini, J. (1994). Client factors influencing group therapy dropout. Psychotherapy, 31(2), 352–361. https://doi.org/10.1037/h0090226
MacNair-Semands, R.R. (2002). Predicting attendance and expectations for group therapy. Group Dynamics: Theory, Research, and Practice, 6(3), 219–228. https://doi.org/10.1037/1089-2699.6.3.219
MacNair-Semands, R.R. (2007). Attending to the spirit of social justice as an ethical approach in group therapy. International Journal of Group Psychotherapy, 57(1), 61–66. https://doi.org/10.1521/ijgp.2007.57.1.61
MacNair-Semands, R.R. (2019). The group therapy questionnaire—short form. University of North Carolina.
MacNair-Semands, R., & Whittingham, M. (Eds.). (2023). Group psychotherapy assessment and practice: A measurement-based care approach. Routledge. https://doi.org/10.4324/9781003255482
McGoldrick, M., & Hardy, K.V. (2019). Re-visioning family therapy: Addressing diversity in clinical practice (3rd ed.). The Guilford Press.
Menakem, R. (2017). My grandmother’s hands: Racialized trauma and the pathway to mending our hearts and bodies. Central Recovery Press.
Miles, J.R., Anders, C., Kivlighan, D.M. III, & Belcher Platt, A.A. (2021). Cultural ruptures: Addressing microaggressions in group therapy. Group Dynamics: Theory, Research, and Practice, 25(1), 74–88. https://doi.org/10.1037/gdn0000149
Motherwell, L., & Shay, J. (Eds.). (2005). Complex dilemmas in group therapy: Pathways to resolution. Routledge.
Nadal, K.L. (2018). Microaggressions and traumatic stress: Theory, research, and clinical treatment. American Psychological Association. https://doi.org/10.1037/0000073-000
Norcross, J.C., & Lambert, M.J. (2018). Psychotherapy relationships that work III. Psychotherapy, 55(4), 303–315. https://doi.org/10.1037/pst0000193
Ogrodniczuk, J.S., Piper, W.E., Joyce, A.S., McCallum, M., & Rosie, J.S. (2003). NEO-five factor personality traits as predictors of response to two forms of group psychotherapy. International Journal of Group Psychotherapy, 53(4), 417–442. https://doi.org/10.1521/ijgp.53.4.417.42832
Ogrodniczuk, J.S., Piper, W.E., & Joyce, A.S. (2004). Differences in men’s and women’s responses to short-term group psychotherapy. Psychotherapy Research, 14(2), 231–243. https://doi.org/10.1093/ptr/kph019
Ormont, L.R. (1992). The leader’s role in resolving resistance and fostering cohesion. Jason Aronson.
Owens, L.R., Syedullah, J., & Williams, R.A.K. (2016). Radical dharma: Talking race, love and liberation. North Atlantic Books.
Piper, W.E., & Perrault, E.L. (1989). Is group therapy effective? A review of empirical research. In H.I. Kaplan & B.J. Sadock (Eds.), Comprehensive group psychotherapy (pp. 285–303). Williams & Wilkins.
Pratt, J.H. (1907). The class method of treating consumption in the homes of the poor. Journal of the American Medical Association, 49(9), 755–759.
Rabinowitz, F.E. (2001). Group therapy for men. In G.R. Brooks & G.E. Good (Eds.), The new handbook of psychotherapy and counseling with men (Vol. 4, pp. 603–621). Jossey-Bass.
Ribeiro, M.D. (Ed.). (2020). Examining social identities and diversity issues in group therapy: Knocking at the boundaries. Routledge. https://doi.org/10.4324/9780429022364
Ribeiro, M.D. (2020). Intersectionality, social identities, and groups examined. In M.D. Ribeiro (Ed.), Examining social identities and diversity issues in group therapy: Knocking at the boundaries (pp. 3–23). Routledge. https://doi.org/10.4324/9780429022364
Ribeiro, M.D. (2021). Intentional call to action: Mindfully discussing race in group psychotherapy. American Journal of Group Psychotherapy, 74(2). https://doi.org/10.1176/appi.psychotherapy.2020004
Ribeiro, M.D., Gross, J.M., & Turner, M.M. (2017). The college counselor’s guide to group psychotherapy. Routledge. https://doi.org/10.4324/9781315545455
Rutan, J.S., Greene, L.R., & Kaklauskas, F.J. (2020a). Preparing to begin a new group. In F.J. Kaklauskas & L.R. Greene (Eds.), Core principles of group psychotherapy: An integrated theory, research, and practice training manual (1st ed., pp. 89–100). Routledge. https://doi.org/10.4324/9780429260803
Rutan, J.S., Greene, L.R., & Kaklauskas, F.J. (2020b). Basic leadership tasks. In F.J. Kaklauskas & L.R. Greene (Eds.), Core principles of group psychotherapy: An integrated theory, research, and practice training manual (1st ed., pp. 111–121). Routledge. https://doi.org/10.4324/9780429260803
Rutan, J.S., & Stone, W.N. (2001). Psychodynamic group psychotherapy. Guilford Press.
Rutan, J.S., Stone, W.N., & Shay, J.J. (2014). Psychodynamic group psychotherapy (4th ed.). Guilford Press.
Singh, A.A., Nassar, S.C., Arredondo, P., & Toporek, R. (2020). The past guides the future: Implementing the multicultural and social justice counseling competencies. Journal of Counseling & Development, 98(3), 238–252. https://doi.org/10.1002/jcad.12319
Smith, T.B., Domenech Rodríguez, M.M., & Bernal, G. (2011). Culture. In J.C. Norcross (Ed.), Psychotherapy relationships that work: Evidence-based responsiveness (pp. 317–335). Oxford University Press. https://doi.org/10.1093/acprof:oso/9780199737208.001.0001
Substance Abuse and Mental Health Services Administration. (2014). SAMHSA’s concept of trauma and guidance for a trauma-informed approach (HHS Publication No. SMA 14-4884). U.S. Department of Health and Human Services. https://store.samhsa.gov/sites/default/files/sma14-4884.pdf
Sue, D.W. (2010). Microaggressions in everyday life: Race, gender, and sexual orientation. John Wiley & Sons, Inc.
Sue, D.W., & Sue, D. (2012). Counseling the culturally diverse: Theory and practice (6th ed.). John Wiley & Sons, Inc.
Sue, D.W., Alsaidi, S., Awad, M.N., Glaeser, E., Calle, C.Z., & Mendez, N. (2019). Disarming racial microaggressions: Microintervention strategies for targets, white allies, and bystanders. American Psychologist, 74(1), 128–142. https://doi.org/10.1037/amp0000296
Sue, D.W., Sue, D., Neville, H.A., & Smith, L. (2019). Counseling the culturally diverse: Theory and practice (8th ed.). John Wiley & Sons, Inc.
Sue, D.W., Sue, D., Neville, H.A., & Smith, L. (2022). Counseling the culturally diverse: Theory and practice (9th ed.). John Wiley & Sons, Inc.
Summers, R.F., & Barber, J.P. (2010). Psychodynamic therapy: A guide to evidence-based practice. Guilford Press.
Tasca, G.A., Cabrera, C., Kristjansson, E., MacNair-Semands, R., Joyce, A.S., & Ogrodniczuk, J.S. (2016). The therapeutic factors inventory-8: Using item response theory to create a brief scale for continuous process monitoring for group psychotherapy. Psychotherapy Research, 26(2), 131–145. https://doi.org/10.1080/10503307.2014.963729
Tasca, G.A., & Maxwell, H. (2021). Attachment and group psychotherapy: Applications to work groups and teams. In C.D. Parks & G.A. Tasca (Eds.), The psychology of groups: The intersection of social psychology and psychotherapy research (pp. 149–167). American Psychological Association. https://doi.org/10.1037/0000201-009
Tasca, G.A., Mikail, S.F., & Hewitt, P.L. (2021). Group psychodynamic-interpersonal psychotherapy. American Psychological Association. https://doi.org/10.1037/0000213-000
Taylor, S.R. (2021). The body is not an apology (2nd ed.). Berrett-Koehler.
Thalmayer, A.G., Toscanelli, C., & Arnett, J.J. (2021). The neglected 95% revisited: Is American psychology becoming less American? American Psychologist, 75(1), 116–129. https://doi.org/10.1037/amp0000622
Tuckman, B.W., & Jensen, M.A.C. (1977). Stages of small-group development revisited. Group and Organizational Studies, 2, 419–427. https://doi.org/10.1177/105960117700200404
Turner, M.M. (2017). Nuts and bolts: The group screen. In M.D. Ribeiro, J. Gross, & M.M. Turner (Eds.), The college counselor’s guide to group psychotherapy (pp. 145–155). Routledge. https://doi.org/10.4324/9781315545455
Valbak, K. (2018). Preparing for group analytic psychotherapy: Meeting the new patient. Group Analysis, 51(2), 159–174. https://doi.org/10.1177/0533316418764385
Wheelan, S.A. (2005). Group processes: A developmental perspective. Pearson Education.
Whittingham, M. (2018). Innovations in group assessment: How focused brief group therapy integrates formal measures to enhance treatment preparation, process, and outcomes. Psychotherapy, 55(2), 186–190. https://doi.org/10.1037/pst0000153
Whittingham, M., Lefforge, N.L., & Marmarosh, C. (2021). Group psychotherapy as a specialty: An inconvenient truth. American Journal of Psychotherapy, 74(2). https://doi.org/10.1176/appi.psychotherapy.20200037
Wright, F., & Gould, L.J. (1996). Research on gender-linked aspects of group behavior: Implications for group psychotherapy. In B. Dechant (Ed.), Women and group psychotherapy: Theory and practice (pp. 333–350). The Guilford Press.
Yalom, I.D., & Leszcz, M. (2020). The theory and practice of group psychotherapy (6th ed.). Basic Books.
Ziadeh, S. (2020). Group interpersonal psychotherapy in the context of poverty and gender: Toward a culturally sound adaption of IPT-G to socioeconomically disadvantaged and depressed Lebanese women. In M.D. Ribeiro (Ed.), Examining social identities and diversity in group therapy: Knocking at the boundaries (pp. 204–222). Routledge. https://doi.org/10.4324/9780429022364